

Effect on Treatment Adherence of Distributing Essential Medicines at No Charge: The CLEAN Meds Randomized Clinical Trial
- PMID: 31589276
- PMCID: PMC6784757
- DOI: 10.1001/jamainternmed.2019.4472
Effect on Treatment Adherence of Distributing Essential Medicines at No Charge: The CLEAN Meds Randomized Clinical Trial
Abstract
Importance: Nonadherence to treatment with medicines is common globally, even for life-saving treatments. Cost is one important barrier to access, and only some jurisdictions provide medicines at no charge to patients.
Objective: To determine whether providing essential medicines at no charge to outpatients who reported not being able to afford medicines improves adherence.
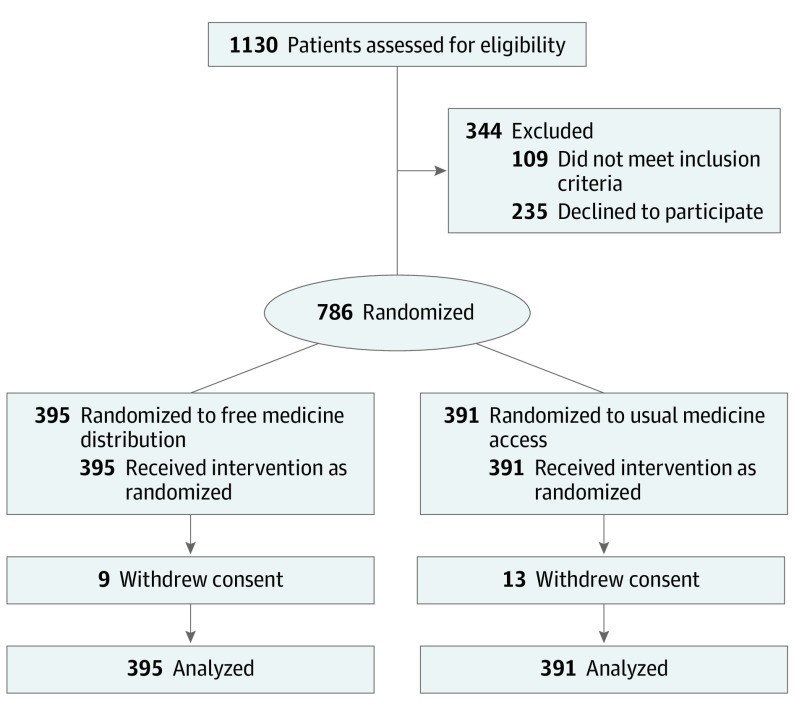
Design, setting, and participants: A multicenter, unblinded, parallel, 2-group, superiority, outcomes assessor-blinded, individually randomized clinical trial conducted at 9 primary care sites in Ontario, Canada, enrolled 786 patients between June 1, 2016, and April 28, 2017, who reported cost-related nonadherence. Follow-up occurred at 12 months. The primary analysis was performed using an intention-to-treat principle.
Interventions: Patients were randomly allocated to receive free medicines on a list of essential medicines in addition to otherwise usual care (n = 395) or usual medicine access and usual care (n = 391).
Main outcomes and measures: The primary outcome was adherence to treatment with all medicines that were appropriately prescribed for 1 year. Secondary outcomes were hemoglobin A1c level, blood pressure, and low-density lipoprotein cholesterol levels 1 year after randomization in participants taking corresponding medicines.
Results: Among the 786 participants analyzed (439 women and 347 men; mean [SD] age, 51.7 [14.3] years), 764 completed the trial. Adherence to treatment with all medicines was higher in those randomized to receive free distribution (151 of 395 [38.2%]) compared with usual access (104 of 391 [26.6%]; difference, 11.6%; 95% CI, 4.9%-18.4%). Control of type 1 and 2 diabetes was not significantly improved by free distribution (hemoglobin A1c, -0.38%; 95% CI, -0.76% to 0.00%), systolic blood pressure was reduced (-7.2 mm Hg; 95% CI, -11.7 to -2.8 mm Hg), and low-density lipoprotein cholesterol levels were not affected (-2.3 mg/dL; 95% CI, -14.7 to 10.0 mg/dL).
Conclusions and relevance: The distribution of essential medicines at no charge for 1 year increased adherence to treatment with medicines and improved some, but not other, disease-specific surrogate health outcomes. These findings could help inform changes to medicine access policies such as publicly funding essential medicines.
Trial registration: ClinicalTrials.gov identifier: NCT02744963.
Conflict of interest statement
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
