

Interfacility Transfer of Medicare Beneficiaries With Acute Type A Aortic Dissection and Regionalization of Care in the United States
- PMID: 31589488
- PMCID: PMC9856243
- DOI: 10.1161/CIRCULATIONAHA.118.038867
Interfacility Transfer of Medicare Beneficiaries With Acute Type A Aortic Dissection and Regionalization of Care in the United States
Abstract
Background: The feasibility and effectiveness of delaying surgery to transfer patients with acute type A aortic dissection-a catastrophic disease that requires prompt intervention-to higher-volume aortic surgery hospitals is unknown. We investigated the hypothesis that regionalizing care at high-volume hospitals for acute type A aortic dissections will lower mortality. We further decomposed this hypothesis into subparts, investigating the isolated effect of transfer and the isolated effect of receiving care at a high-volume versus a low-volume facility.
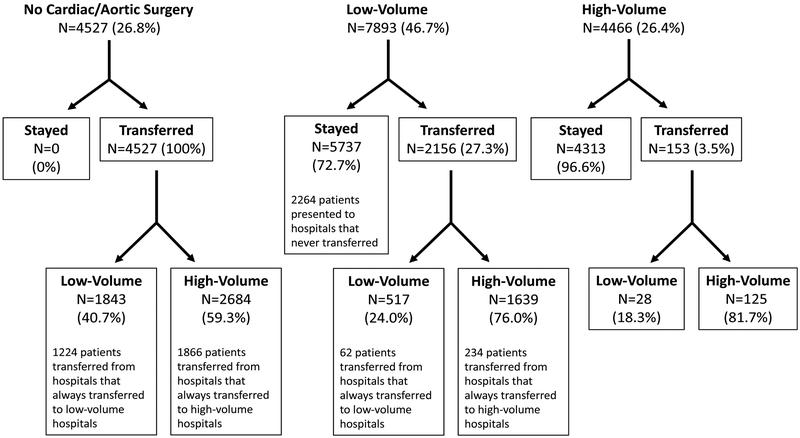
Methods: We compared the operative mortality and long-term survival between 16 886 Medicare beneficiaries diagnosed with an acute type A aortic dissection between 1999 and 2014 who (1) were transferred versus not transferred, (2) underwent surgery at high-volume versus low-volume hospitals, and (3) were rerouted versus not rerouted to a high-volume hospital for treatment. We used a preference-based instrumental variable design to address unmeasured confounding and matching to separate the effect of transfer from volume.
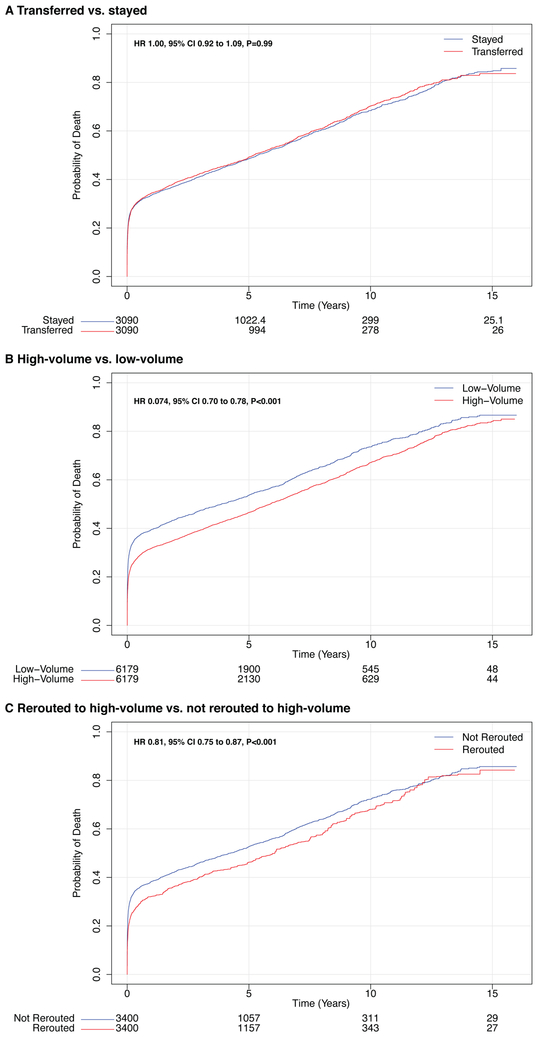
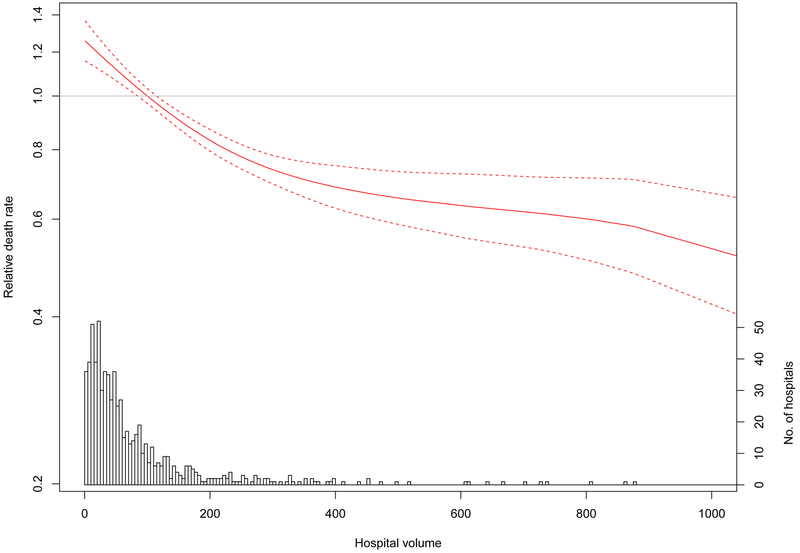
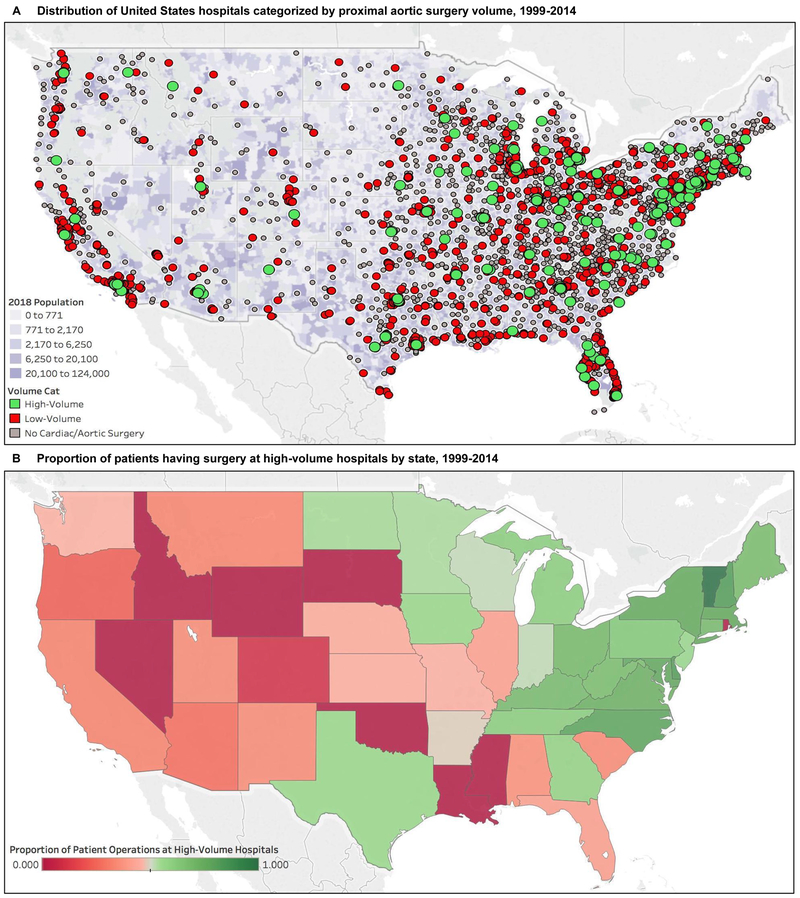
Results: Between 1999 and 2014, 40.5% of patients with an acute type A aortic dissection were transferred, and 51.9% received surgery at a high-volume hospital. Interfacility transfer was not associated with a change in operative mortality (risk difference, -0.69%; 95% CI, -2.7% to 1.35%) or long-term mortality. Despite delaying surgery, a regionalization policy that transfers patients to high-volume hospitals was associated with a 7.2% (95% CI, 4.1%-10.3%) absolute risk reduction in operative mortality; this association persisted in the long term (hazard ratio, 0.81; 95% CI, 0.75-0.87). The median distance needed to reroute each patient to a high-volume hospital was 50.1 miles (interquartile range, 12.4-105.4 miles).
Conclusions: Operative and long-term mortality were substantially reduced in patients with acute type A aortic dissection who were rerouted to high-volume hospitals. Policy makers should evaluate the feasibility and benefits of regionalizing the surgical treatment of acute type A aortic dissection in the United States.
Keywords: aneurysm, dissecting; causality; confounding factors, epidemiology; epidemiology; patient transfer; surgery.
Figures
Comment in
-
Introduction to the 2019 Cardiovascular Surgery-Themed Issue.Circulation. 2019 Oct 8;140(15):1231-1232. doi: 10.1161/CIRCULATIONAHA.119.043795. Epub 2019 Oct 7. Circulation. 2019. PMID: 31589489 No abstract available.
-
Access or excess? Examining the argument for regionalized cardiac care.J Thorac Cardiovasc Surg. 2020 Sep;160(3):813-819. doi: 10.1016/j.jtcvs.2019.12.125. Epub 2020 May 29. J Thorac Cardiovasc Surg. 2020. PMID: 32475504 No abstract available.
References
-
- Clouse WD, Hallett JW Jr., Schaff HV, Spittell PC, Rowland CM, Ilstrup DM Melton LJ 3rd. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc. 2004;79:176–80. - PubMed
-
- Meszaros I, Morocz J, Szlavi J, Schmidt J, Tornoci L, Nagy L Szep L. Epidemiology and clinicopathology of aortic dissection. Chest. 2000;117:1271–8. - PubMed
-
- Daily PO, Trueblood HW, Stinson EB, Wuerflein RD Shumway NE. Management of acute aortic dissections. Ann Thorac Surg. 1970;10:237–47. - PubMed
-
- Nienaber CA Clough RE. Management of acute aortic dissection. Lancet. 2015;385:800–11. - PubMed
-
- Hirst AE Jr., Johns VJ Jr. Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine (Baltimore). 1958;37:217–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
