

Treatment Patterns and Medication Use in Patients with Postherpetic Neuralgia
- PMID: 31589557
- PMCID: PMC10398040
- DOI: 10.18553/jmcp.2019.19093
Treatment Patterns and Medication Use in Patients with Postherpetic Neuralgia
Abstract
Background: Postherpetic neuralgia (PHN) is a chronic, painful condition characterized by persistent pain following resolution of a herpes zoster (HZ) infection. Epidemiologic data demonstrate that the risks for HZ infections and the development of PHN increase with age.
Objective: To characterize prescribing patterns, health care utilization, and treatment costs for adults with PHN based on real-world data.
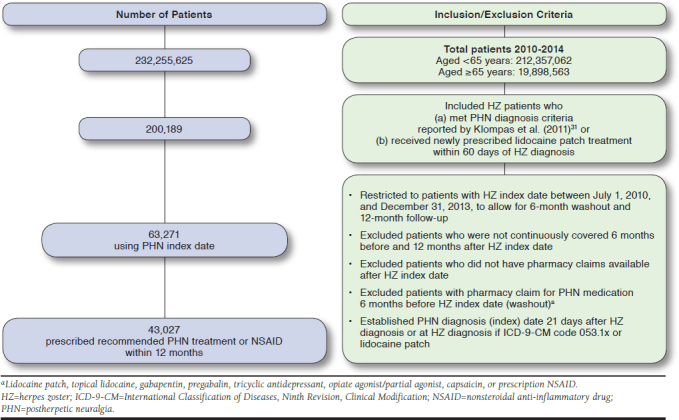
Methods: This study analyzed medical and pharmacy claims from 2010 to 2014 in the MarketScan Commercial and Medicare Supplemental databases. PHN patients were identified based on criteria from a published algorithm. PHN treatment patterns were analyzed by age and reported descriptively for patients aged < 65 or ≥ 65 years. Excess incremental health care costs were calculated for PHN patients by comparing expenditures for a cohort of PHN patients to expenditures of a propensity score-matched control group of patients with HZ alone.
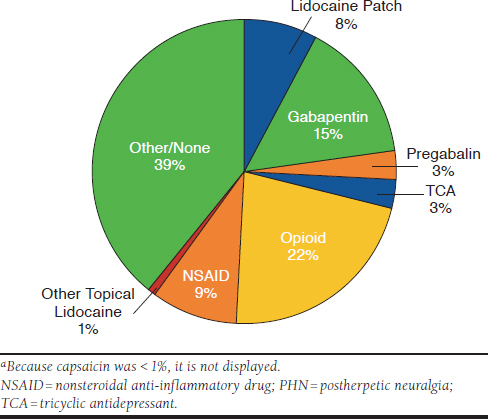
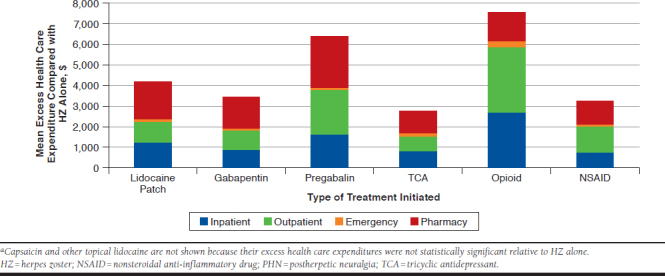
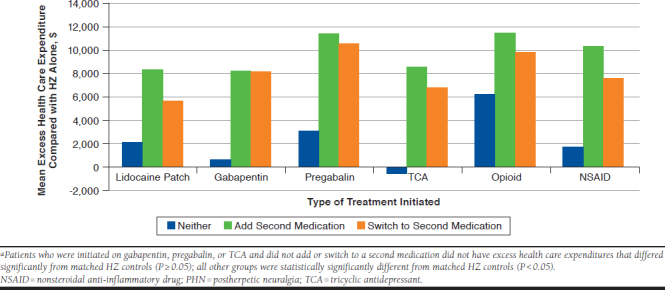
Results: Approximately 0.4% of patients aged < 65 years were diagnosed with HZ versus 1.3% of patients aged ≥ 65 years; approximately 15.3% of HZ patients aged < 65 years and 26.4% of patients aged ≥ 65 years were diagnosed with PHN. Overall, opioids remained the most frequently prescribed initial treatment. Approximately 21.6% of PHN patients received an opioid as an initial treatment for PHN, 15.1% received gabapentin; 8.9% received a prescription nonsteroidal anti-inflammatory drug (NSAID); 8.3% received a lidocaine patch; 3.3% received pregabalin; 2.5% received a tricyclic antidepressants (TCAs); 0.8% received other topical lidocaine; and < 1% received capsaicin. Observed first-line use of the lidocaine patch and gabapentin was higher in patients aged ≥ 65 years relative to patients aged < 65 years. When separated by age group, only 24.6% of patients aged < 65 years and 38.5% of patients aged ≥ 65 years were prescribed a recommended first-line treatment for initial PHN therapy (gabapentin, lidocaine patch, pregabalin, and TCAs). Comparisons of treatment costs of PHN patients to matched HZ patients without PHN indicated that PHN patients initiated on opioids had the highest mean additional health care expenditure compared with PHN patients initiated on other medications. On average, PHN patients initiated on opioids had $7,601 additional health care expenditure compared with HZ patients with no PHN; additional expenditures were $6,428 for pregabalin, $4,213 for lidocaine patches, $3,478 for gabapentin, $3,304 for NSAIDs, and $2,797 for TCAs, respectively.
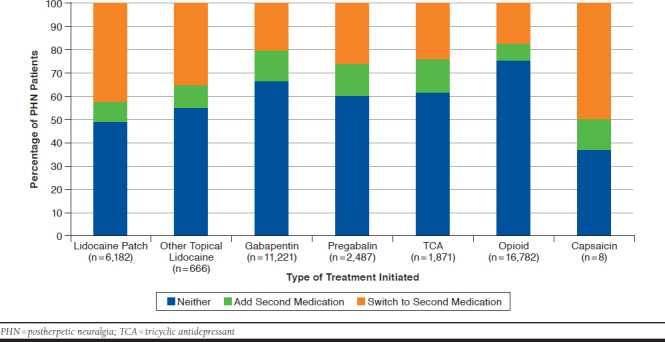
Conclusions: Management of PHN is associated with substantial utilization of opioid-based therapies across all ages. Medications supported by evidence either as first-line therapies or as part of a multimodal regimen for the management of PHN are underused relative to opioid-based PHN therapies. Improving adherence to evidence-based PHN treatment regimens offers the potential to reduce opioid prescribing first line and reduce overall treatment costs. Given the emphasis to reduce opioid prescribing to minimize the risk of dependence, abuse, and diversion, multimodal analgesic treatments that can avoid or reduce opioid use should be considered.
Disclosures: Research funding was provided by SCILEX Pharmaceuticals. The sponsor reviewed and approved the research plan and provided support for manuscript preparation through Patel's role as a coauthor of this manuscript. The sponsor's product (lidocaine patch) was not used in this study. Patel is a paid employee of SCILEX Pharmaceuticals. Goss is an employee and minority owner of Boston Healthcare Associates, which received a research grant from SCILEX Pharmaceuticals to conduct this study. Gudin reports advisory board fees from AcelRx Pharmaceuticals and BioDelivery Sciences International and consulting fees from Averitas, Daiichi, Hisumitsu, Nektar, Purdue, Quest Diagnostics, SCILEX Pharmaceuticals, and US WorldMeds, unrelated to this study. Fudin reports advisory board fees from AcelRx Pharmaceuticals, Human Half-Cell, Quest Diagnostics, GlaxoSmithKline, SCILEX Pharmaceuticals, BioDelivery Sciences, Daiichi Sankyo, and Salix Pharmaceuticals; speaker fees from Daiichi Sankyo, Salix Pharmaceuticals, Abbott Laboratories, Acutis Diagnostics, and AstraZeneca; and consulting fees from Firstox Laboratories, unrelated to this study. The other authors have nothing to disclose. Parts of this research were presented at the AMCP Managed Care & Specialty Pharmacy Annual Meeting; April 22, 2016; San Francisco, CA, and at the 35th Annual Scientific Meeting of the American Pain Society; May 11-14, 2016; Austin, TX.
Conflict of interest statement
Research funding was provided by SCILEX Pharmaceuticals. The sponsor reviewed and approved the research plan and provided support for manuscript preparation through Patel’s role as a coauthor of this manuscript. The sponsor’s product (lidocaine patch) was not used in this study.
Patel is a paid employee of SCILEX Pharmaceuticals. Goss is an employee and minority owner of Boston Healthcare Associates, which received a research grant from SCILEX Pharmaceuticals to conduct this study. Gudin reports advisory board fees from AcelRx Pharmaceuticals and BioDelivery Sciences International and consulting fees from Averitas, Daiichi, Hisumitsu, Nektar, Purdue, Quest Diagnostics, SCILEX Pharmaceuticals, and US WorldMeds, unrelated to this study. Fudin reports advisory board fees from AcelRx Pharmaceuticals, Human Half-Cell, Quest Diagnostics, GlaxoSmithKline, SCILEX Pharmaceuticals, BioDelivery Sciences, Daiichi Sankyo, and Salix Pharmaceuticals; speaker fees from Daiichi Sankyo, Salix Pharmaceuticals, Abbott Laboratories, Acutis Diagnostics, and AstraZeneca; and consulting fees from Firstox Laboratories, unrelated to this study. The other authors have nothing to disclose.
Parts of this research were presented at the AMCP Managed Care & Specialty Pharmacy Annual Meeting; April 22, 2016; San Francisco, CA, and at the 35th Annual Scientific Meeting of the American Pain Society; May 11-14, 2016; Austin, TX.
Figures
Similar articles
-
Comparing healthcare costs of Medicaid patients with postherpetic neuralgia (PHN) treated with lidocaine patch 5% versus gabapentin or pregabalin.J Med Econ. 2010;13(3):482-91. doi: 10.3111/13696998.2010.506176. J Med Econ. 2010. PMID: 20684669
-
Treatment patterns of postherpetic neuralgia patients before and after the launch of pregabalin and its effect on medical costs: Analysis of Japanese claims data provided by Japan Medical Data Center.J Dermatol. 2017 Jul;44(7):767-773. doi: 10.1111/1346-8138.13784. Epub 2017 Mar 3. J Dermatol. 2017. PMID: 28256737
-
A retrospective evaluation of the use of gabapentin and pregabalin in patients with postherpetic neuralgia in usual-care settings.Clin Ther. 2007 Aug;29(8):1655-70. doi: 10.1016/j.clinthera.2007.08.019. Clin Ther. 2007. PMID: 17919547
-
Postherpetic Neuralgia: Current Evidence on the Topical Film-Forming Spray with Bupivacaine Hydrochloride and a Review of Available Treatment Strategies.Adv Ther. 2020 May;37(5):2003-2016. doi: 10.1007/s12325-020-01335-9. Epub 2020 Apr 15. Adv Ther. 2020. PMID: 32297285 Free PMC article. Review.
-
Diagnosing and managing postherpetic neuralgia.Drugs Aging. 2012 Nov;29(11):863-9. doi: 10.1007/s40266-012-0014-3. Drugs Aging. 2012. PMID: 23038608 Free PMC article. Review.
Cited by
-
Transcriptome Analysis Reveals the Role of Cellular Calcium Disorder in Varicella Zoster Virus-Induced Post-Herpetic Neuralgia.Front Mol Neurosci. 2021 May 17;14:665931. doi: 10.3389/fnmol.2021.665931. eCollection 2021. Front Mol Neurosci. 2021. PMID: 34079439 Free PMC article.
-
Trazodone once-a-day: A formula for addressing challenges in antidepressant safety and tolerability.Neurosci Appl. 2023 May 22;2:101127. doi: 10.1016/j.nsa.2023.101127. eCollection 2023. Neurosci Appl. 2023. PMID: 40655971 Free PMC article. Review.
-
Bioinformatics Analysis of Genes and Mechanisms in Postherpetic Neuralgia.Pain Res Manag. 2020 Sep 24;2020:1380504. doi: 10.1155/2020/1380504. eCollection 2020. Pain Res Manag. 2020. PMID: 33029266 Free PMC article.
-
Topical Lidocaine for Chronic Pain Treatment.Drug Des Devel Ther. 2021 Sep 29;15:4091-4103. doi: 10.2147/DDDT.S328228. eCollection 2021. Drug Des Devel Ther. 2021. PMID: 34616143 Free PMC article. Review.
-
Nonprescription Products of Internet Retailers for the Prevention and Management of Herpes Zoster and Postherpetic Neuralgia: Analysis of Consumer Reviews on Amazon.JMIR Dermatol. 2021 Feb 8;4(1):e24971. doi: 10.2196/24971. JMIR Dermatol. 2021. PMID: 37632802 Free PMC article.
References
-
- Adams EN, Parnapy S, Bautista P. Herpes zoster and vaccination: a clinical review. Am J Health Syst Pharm. 2010;67(9):724-27. - PubMed
-
- Leung J, Harpaz R, Molinari NA, Jumaan A, Zhou F. Herpes zoster incidence among insured persons in the United States, 1993-2006: evaluation of the impact of varicella vaccination. Clin Infect Dis. 2011;52(3):332-40. - PubMed
-
- Oxman MN, Levin MJ, Johnson GR, et al. ; Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271-84. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
