

The Neurocognitive Assessment in the Metabolic and Aging Cohort (NAMACO) study: baseline participant profile
- PMID: 31589807
- PMCID: PMC6916574
- DOI: 10.1111/hiv.12795
The Neurocognitive Assessment in the Metabolic and Aging Cohort (NAMACO) study: baseline participant profile
Abstract
Objectives: The aim of the study was to examine baseline neurocognitive impairment (NCI) prevalence and factors associated with NCI among patients enrolled in the Neurocognitive Assessment in the Metabolic and Aging Cohort (NAMACO) study.
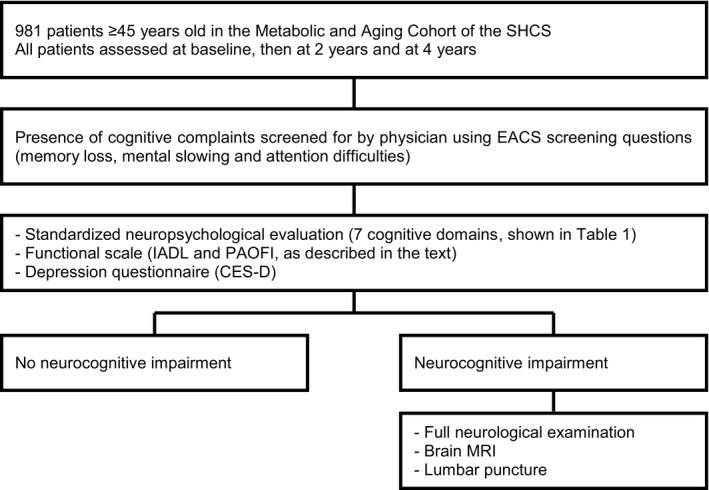
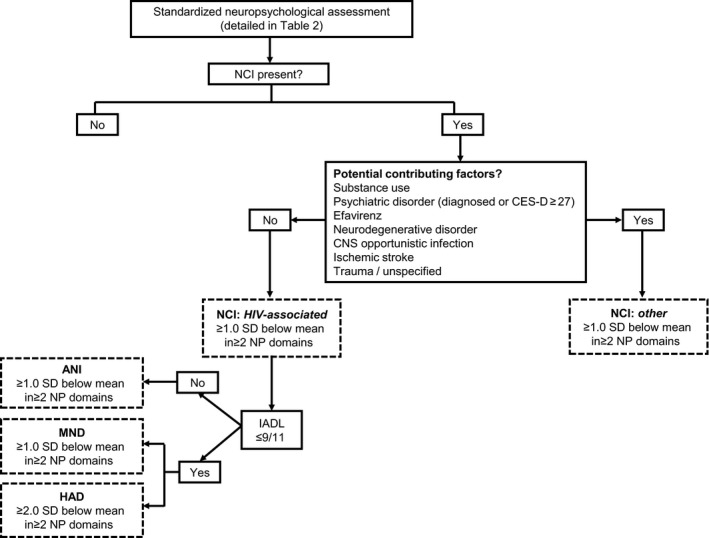
Methods: The NAMACO study is an ongoing, prospective, longitudinal, multicentre and multilingual (German, French and Italian) study within the Swiss HIV Cohort Study. Between 1 May 2013 and 30 November 2016, 981 patients ≥ 45 years old were enrolled in the study. All underwent standardized neuropsychological (NP) assessment by neuropsychologists. NCI was diagnosed using Frascati criteria and classified as HIV-associated or as related to other factors. Dichotomized analysis (NCI versus no NCI) and continuous analyses (based on NP test z-score means) were performed.
Results: Most patients (942; 96.2%) had viral loads < 50 HIV-1 RNA copies/mL. NCI was identified in 390 patients (39.8%): 263 patients (26.8%) had HIV-associated NCI [249 patients (25.4%) had asymptomatic neurocognitive impairment (ANI)] and 127 patients (13%) had NCI attributable to other factors, mainly psychiatric disorders. There was good correlation between dichotomized and continuous analyses, with NCI associated with older age, non-Caucasian ethnicity, shorter duration of education, unemployment and longer antiretroviral therapy duration.
Conclusions: In this large sample of aging people living with HIV with well-controlled infection in Switzerland, baseline HIV-associated NCI prevalence, as diagnosed after formal NP assessment, was 26.8%, with most cases being ANI. The NAMACO study data will enable longitudinal analyses within this population to examine factors affecting NCI development and course.
Keywords: HIV-associated neurocognitive disorder; aging; neurocognitive impairment; neuropsychological testing.
© 2019 The Authors. HIV Medicine published by John Wiley & Sons Ltd on behalf of British HIV Association.
Figures
References
-
- McArthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. Lancet Neurol 2005; 4: 543–555. - PubMed
-
- Bhaskaran K, Mussini C, Antinori A et al Changes in the incidence and predictors of human immunodeficiency virus‐associated dementia in the era of highly active antiretroviral therapy. Ann Neurol 2008; 63: 213–221. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
