

Efficacy and safety of first line treatments for patients with advanced epidermal growth factor receptor mutated, non-small cell lung cancer: systematic review and network meta-analysis
- PMID: 31591158
- PMCID: PMC6778694
- DOI: 10.1136/bmj.l5460
Efficacy and safety of first line treatments for patients with advanced epidermal growth factor receptor mutated, non-small cell lung cancer: systematic review and network meta-analysis
Abstract
Objective: To compare the efficacy and safety of first line treatments for patients with advanced epidermal growth factor receptor (EGFR) mutated non-small cell lung cancer (NSCLC).
Design: Systematic review and network meta-analysis.
Data sources: PubMed, Embase, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, and several international conference databases, from inception to 20 May 2019.
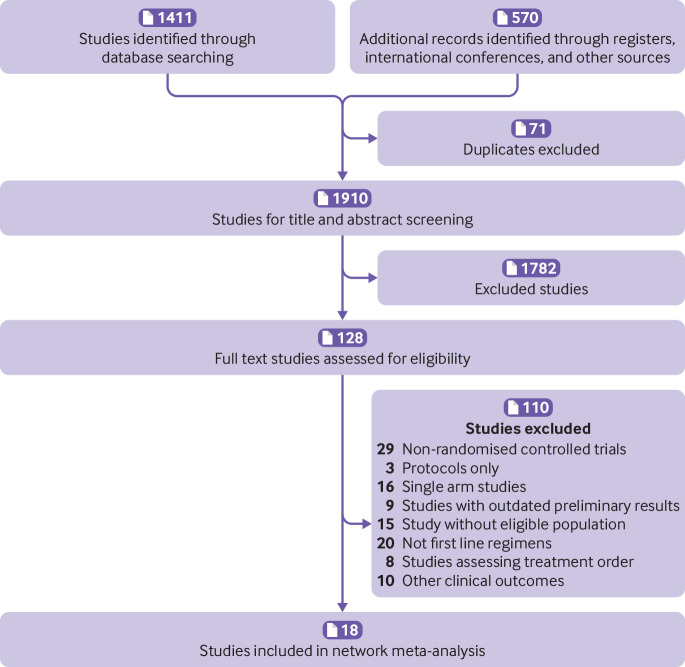
Eligibility criteria for selecting studies: Published and unpublished randomised controlled trials comparing two or more treatments in the first line setting for patients with advanced EGFR mutated NSCLC were included in a bayesian network meta-analysis. Eligible studies reported at least one of the following clinical outcome measures: progression free survival, overall survival, objective response rate, and adverse events of grade 3 or higher.
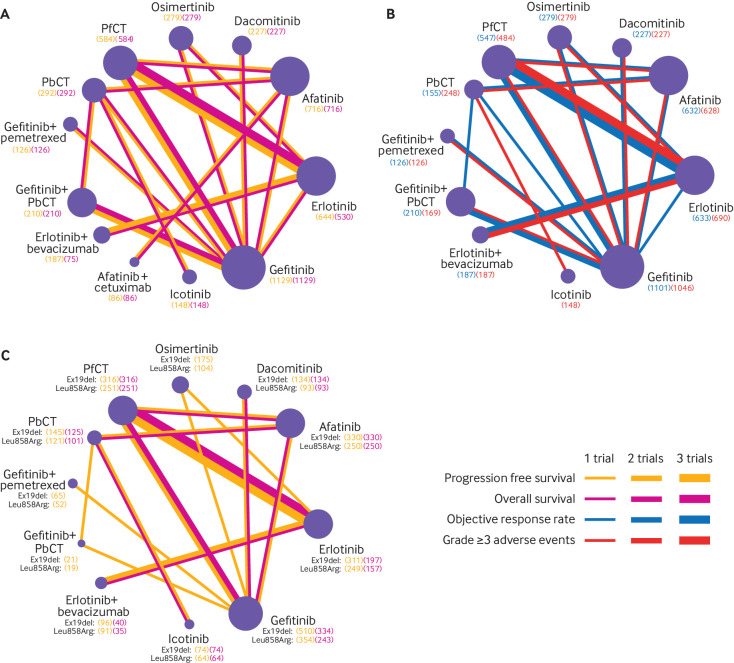
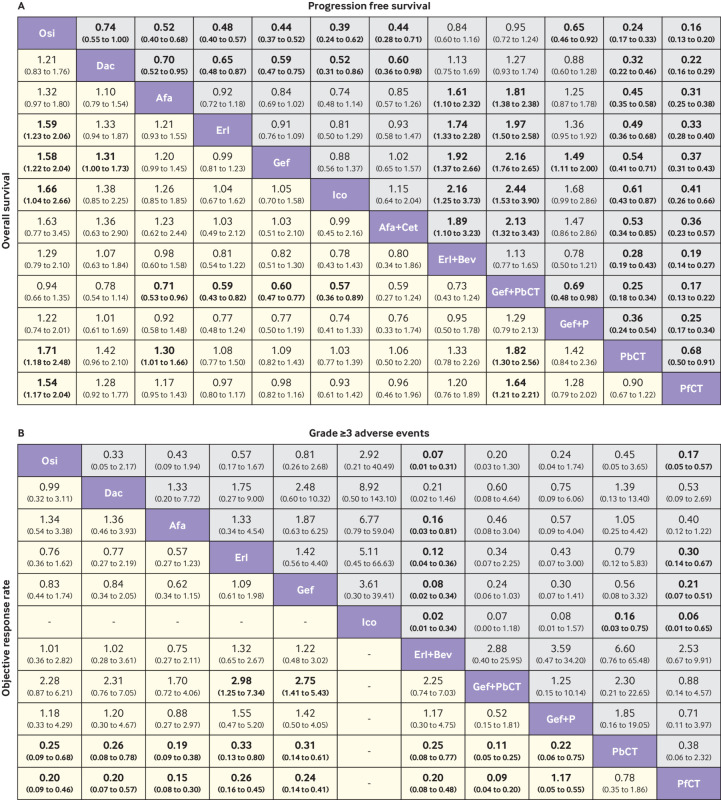
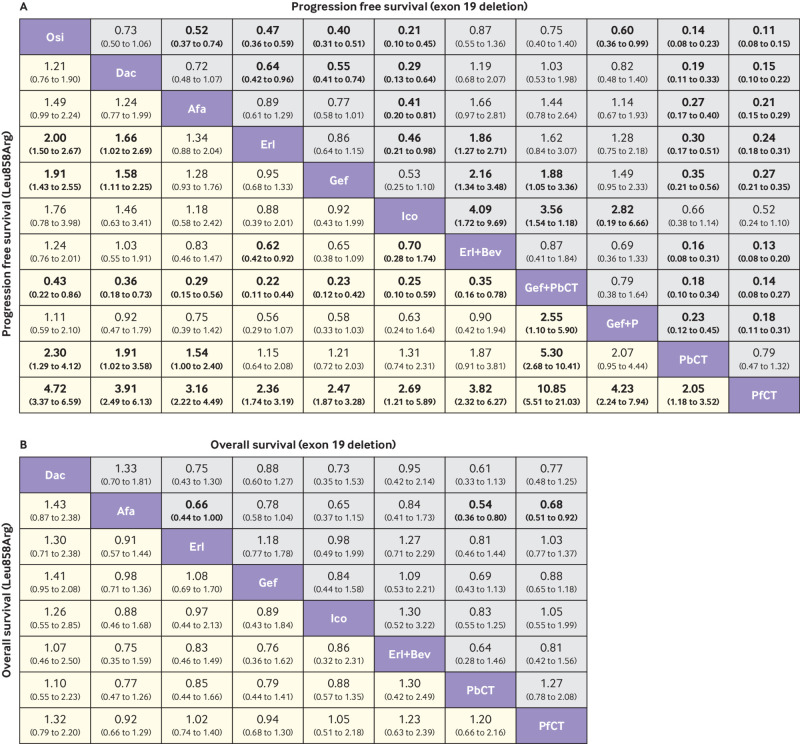
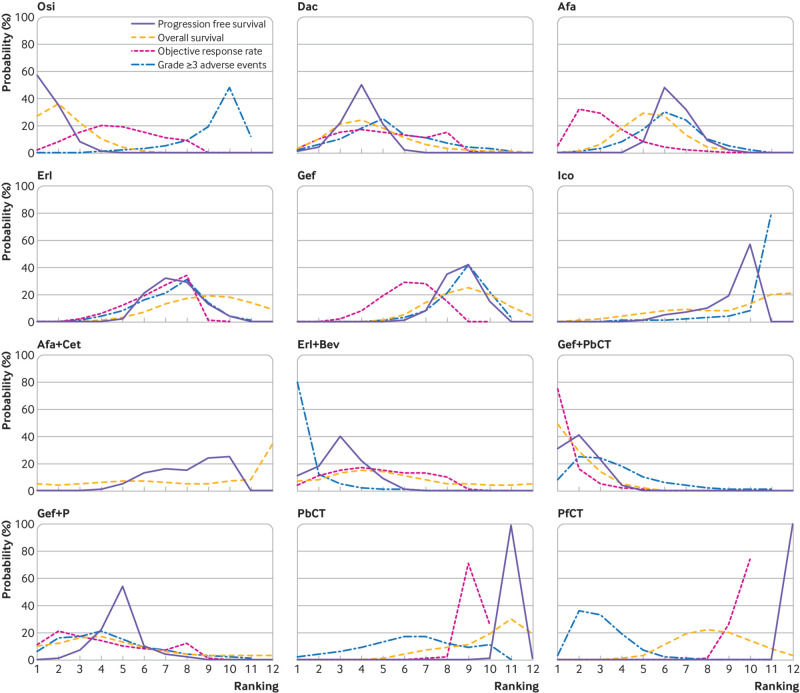
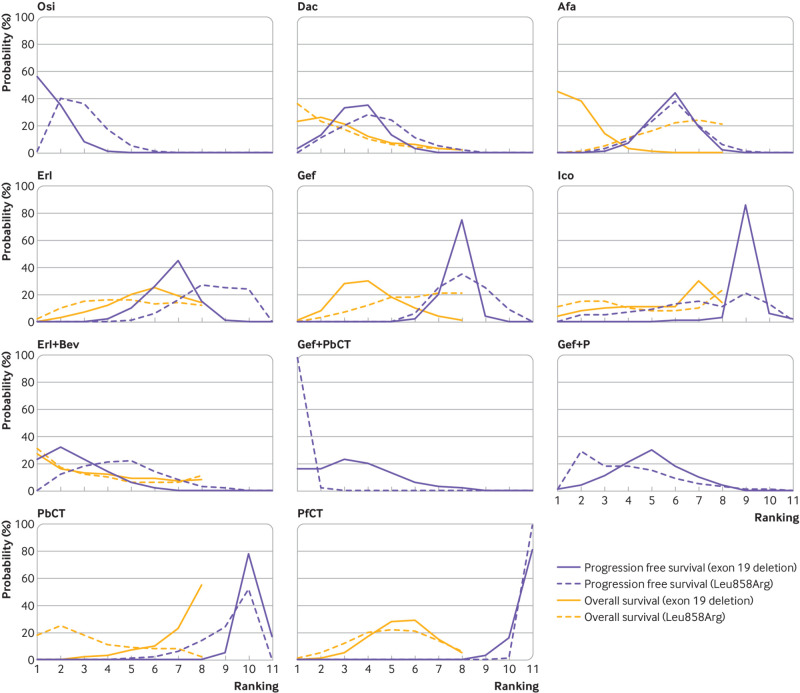
Results: 18 eligible trials involved 4628 patients and 12 treatments: EGFR tyrosine kinase inhibitors (TKIs; osimertinib, dacomitinib, afatinib, erlotinib, gefitinib, and icotinib), pemetrexed based chemotherapy, pemetrexed free chemotherapy, and combination treatments (afatinib plus cetuximab, erlotinib plus bevacizumab, gefitinib plus pemetrexed based chemotherapy, and gefitinib plus pemetrexed). Consistent with gefitinib plus pemetrexed based chemotherapy (hazard ratio 0.95, 95% credible interval 0.72 to 1.24), osimertinib showed the most favourable progression free survival, with significant differences versus dacomitinib (0.74, 0.55 to 1.00), afatinib (0.52, 0.40 to 0.68), erlotinib (0.48, 0.40 to 0.57), gefitinib (0.44, 0.37 to 0.52), icotinib (0.39, 0.24 to 0.62), pemetrexed based chemotherapy (0.24, 0.17 to 0.33), pemetrexed free chemotherapy (0.16, 0.13 to 0.20), afatinib plus cetuximab (0.44, 0.28 to 0.71), and gefitinib plus pemetrexed (0.65, 0.46 to 0.92). Osimertinib and gefitinib plus pemetrexed based chemotherapy were also consistent (0.94, 0.66 to 1.35) in providing the best overall survival benefit. Combination treatments caused more toxicity in general, especially erlotinib plus bevacizumab, which caused the most adverse events of grade 3 or higher. Different toxicity spectrums were revealed for individual EGFR-TKIs. Subgroup analyses by the two most common EGFR mutation types indicated that osimertinib was associated with the best progression free survival in patients with the exon 19 deletion, and gefitinib plus pemetrexed based chemotherapy was associated with the best progression free survival in patients with the Leu858Arg mutation.
Conclusions: These results indicate that osimertinib and gefitinib plus pemetrexed based chemotherapy were associated with the best progression free survival and overall survival benefits for patients with advanced EGFR mutated NSCLC, compared with other first line treatments. The treatments resulting in the best progression free survival for patients with the exon 19 deletion and Leu858Arg mutations were osimertinib and gefitinib plus pemetrexed based chemotherapy, respectively.
Systematic review registration: PROSPERO CRD42018111954.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- NCCN clinical practice guidelines in oncology for non-small cell lung cancer. Version 2. 2019. https://www.nccn.org/patients. Accessed 21 November 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous