

Towards precision oncology in advanced prostate cancer
- PMID: 31591549
- PMCID: PMC6858516
- DOI: 10.1038/s41585-019-0237-8
Towards precision oncology in advanced prostate cancer
Abstract
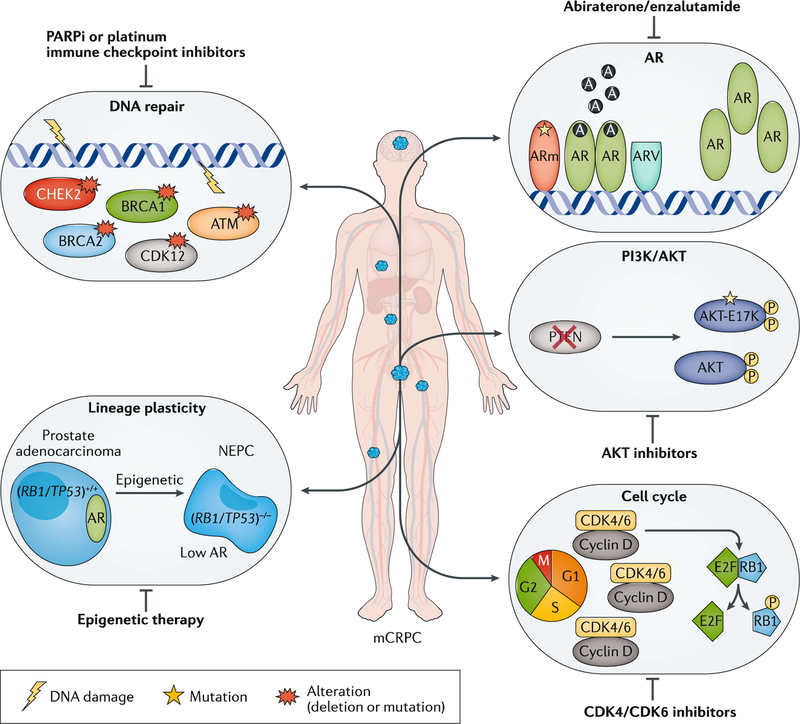
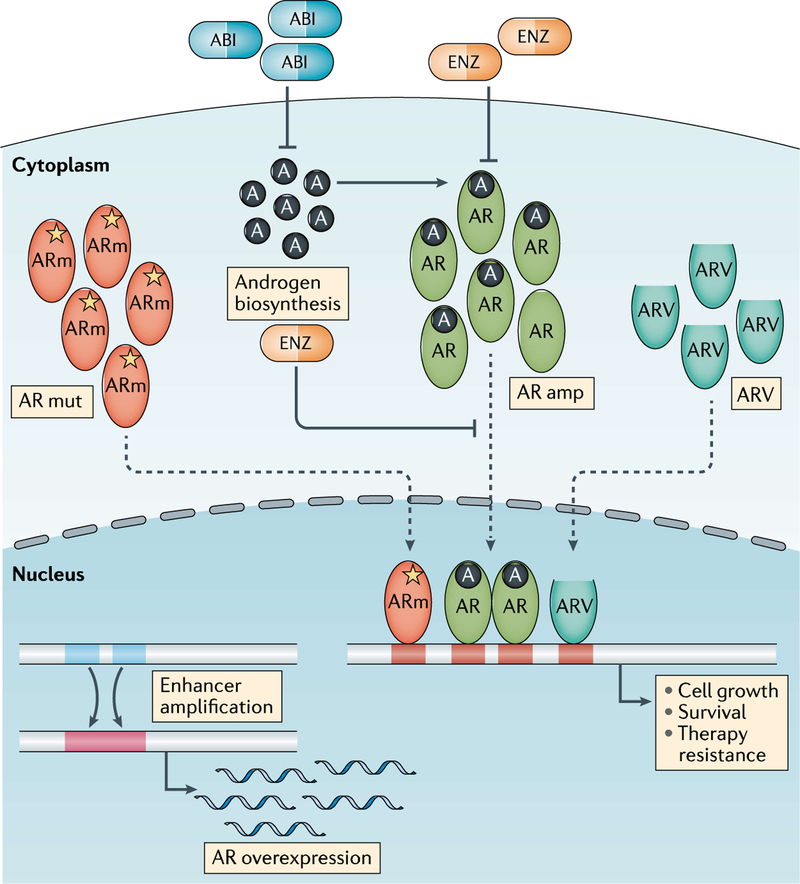
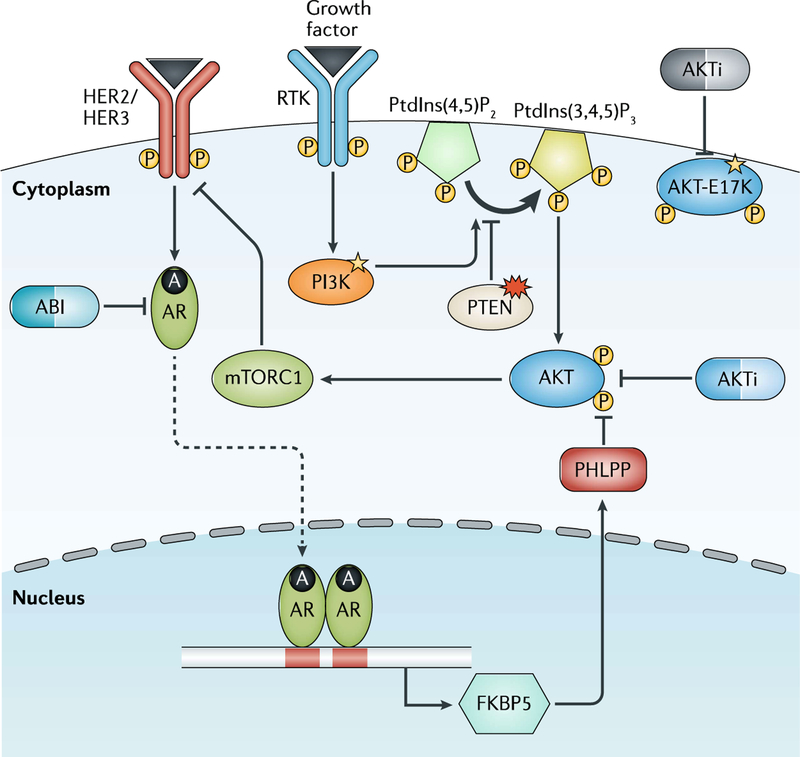
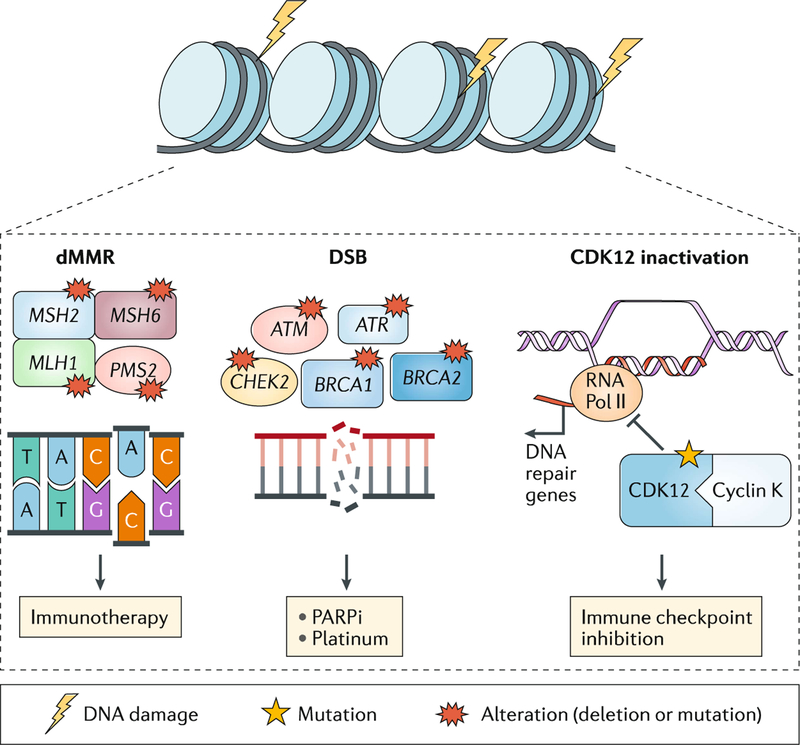
Metastatic biopsy programmes combined with advances in genomic sequencing have provided new insights into the molecular landscape of castration-resistant prostate cancer (CRPC), identifying actionable targets, and emerging resistance mechanisms. The detection of DNA repair aberrations, such as mutation of BRCA2, could help select patients for poly(ADP-ribose) polymerase (PARP) inhibitor or platinum chemotherapy, and mismatch repair gene defects and microsatellite instability have been associated with responses to checkpoint inhibitor immunotherapy. Poor prognostic features, such as the presence of RB1 deletion, might help guide future therapeutic strategies. Our understanding of the molecular features of CRPC is now being translated into the clinic in the form of increased molecular testing for use of these agents and for clinical trial eligibility. Genomic testing offers opportunities for improving patient selection for systemic therapies and, ultimately, patient outcomes. However, challenges for precision oncology in advanced prostate cancer still remain, including the contribution of tumour heterogeneity, the timing and potential cooperation of multiple driver gene aberrations, and diverse resistant mechanisms. Defining the optimal use of molecular biomarkers in the clinic, including tissue-based and liquid biopsies, is a rapidly evolving field.
Figures
References
-
- Ferlay J et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 136, E359–E386 (2015). - PubMed
-
- Siegel RL, Miller KD & Jemal A Cancer statistics, 2019. CA Cancer J. Clin 69, 7–34 (2019). - PubMed
-
- Huggins C & Hodges CV Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. CA Cancer J. Clin 22,232–240(1972). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
