

A rectal cancer organoid platform to study individual responses to chemoradiation
- PMID: 31591597
- PMCID: PMC7385919
- DOI: 10.1038/s41591-019-0584-2
A rectal cancer organoid platform to study individual responses to chemoradiation
Abstract
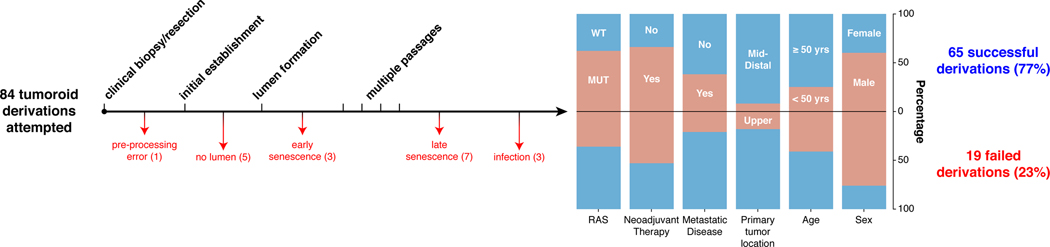
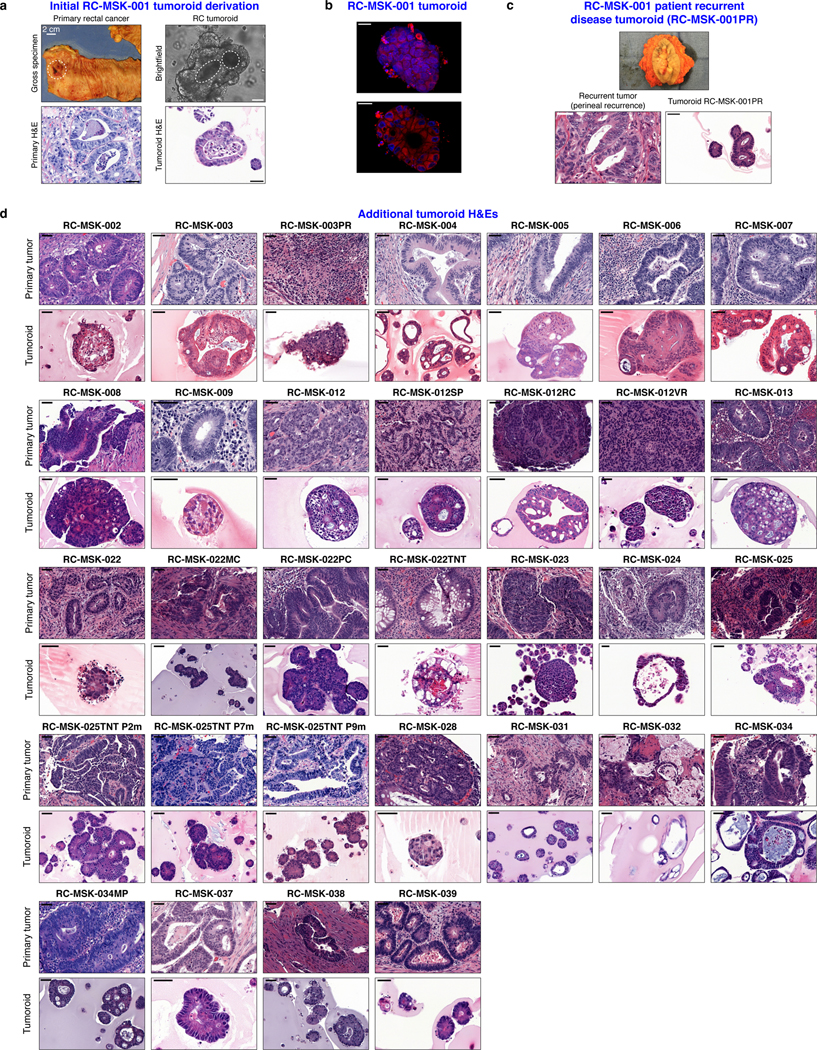
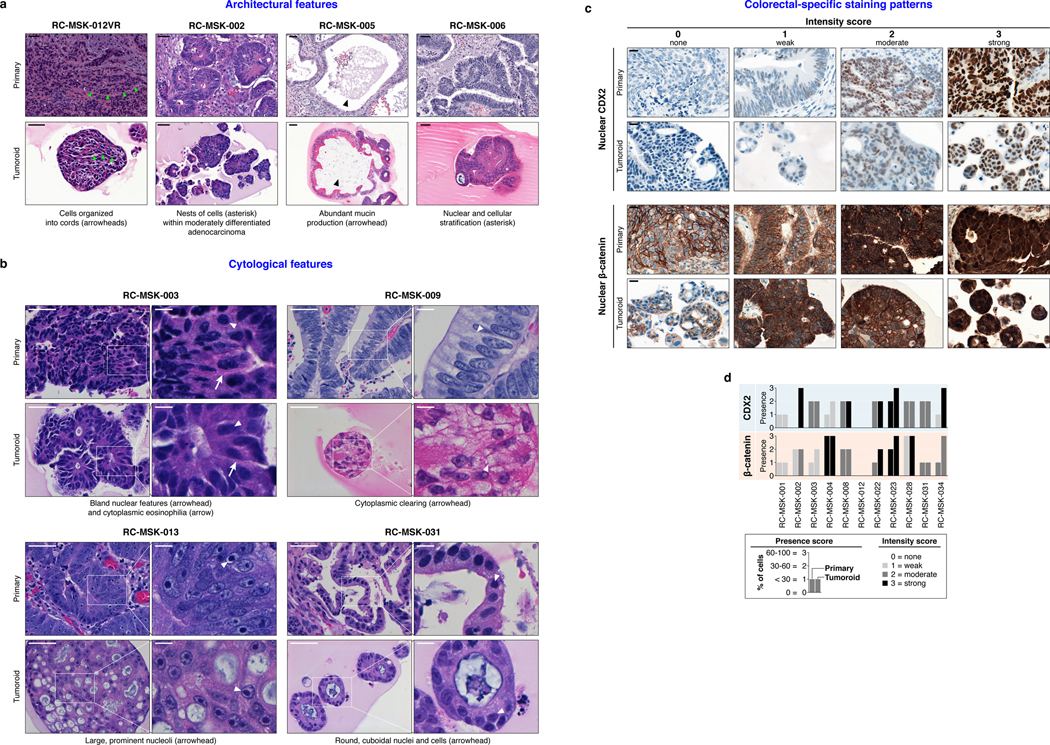
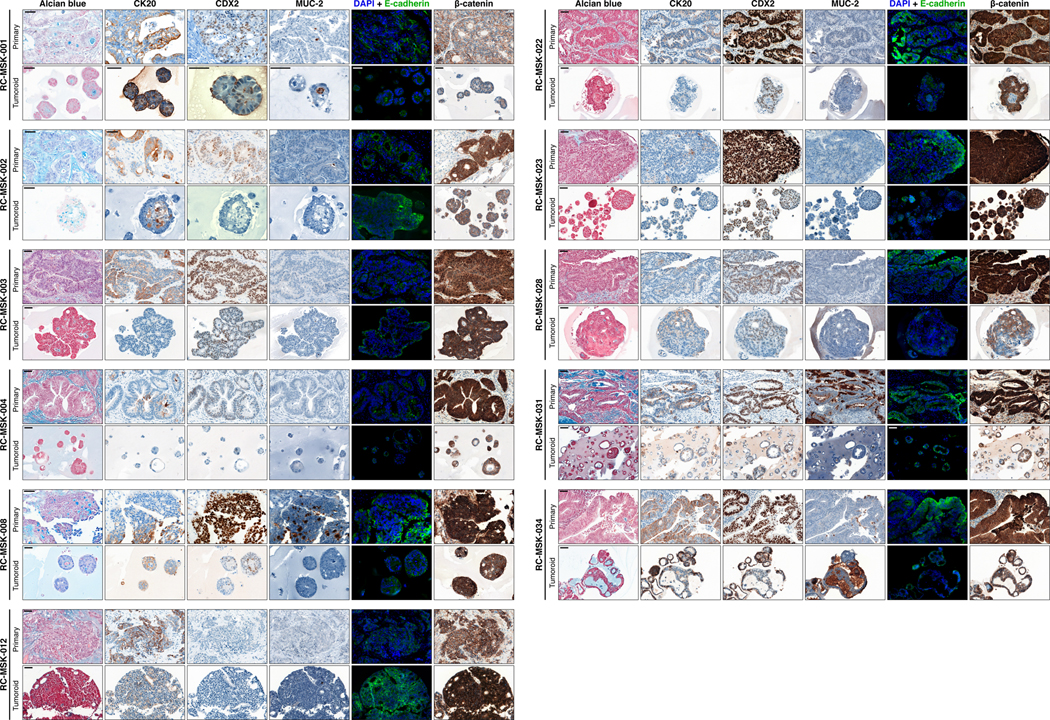
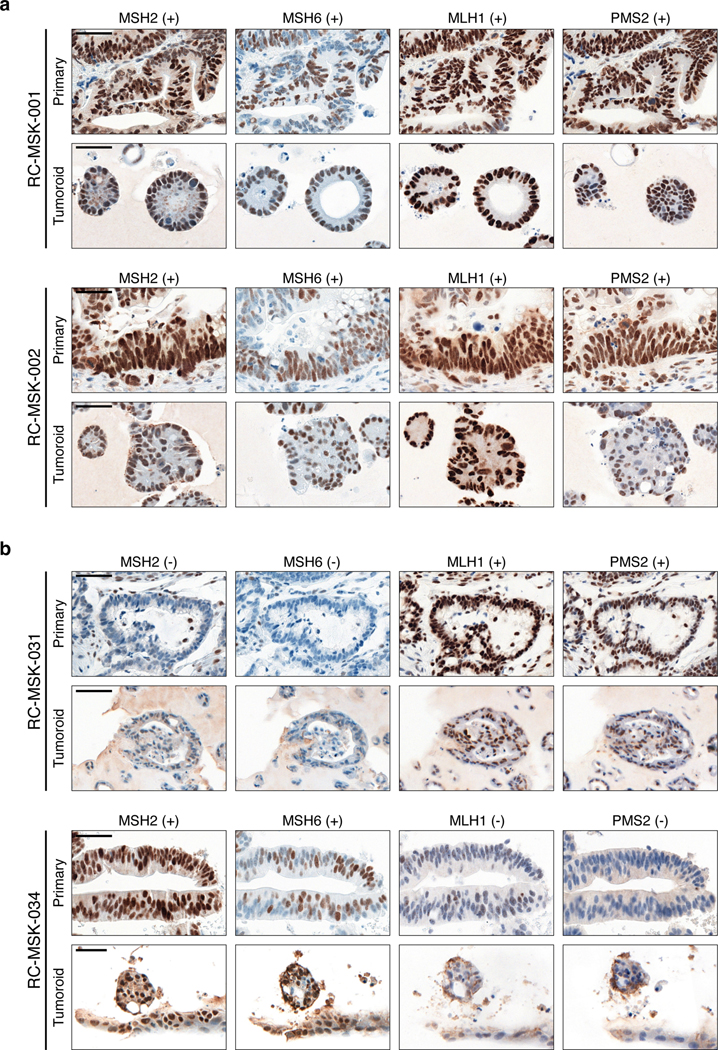
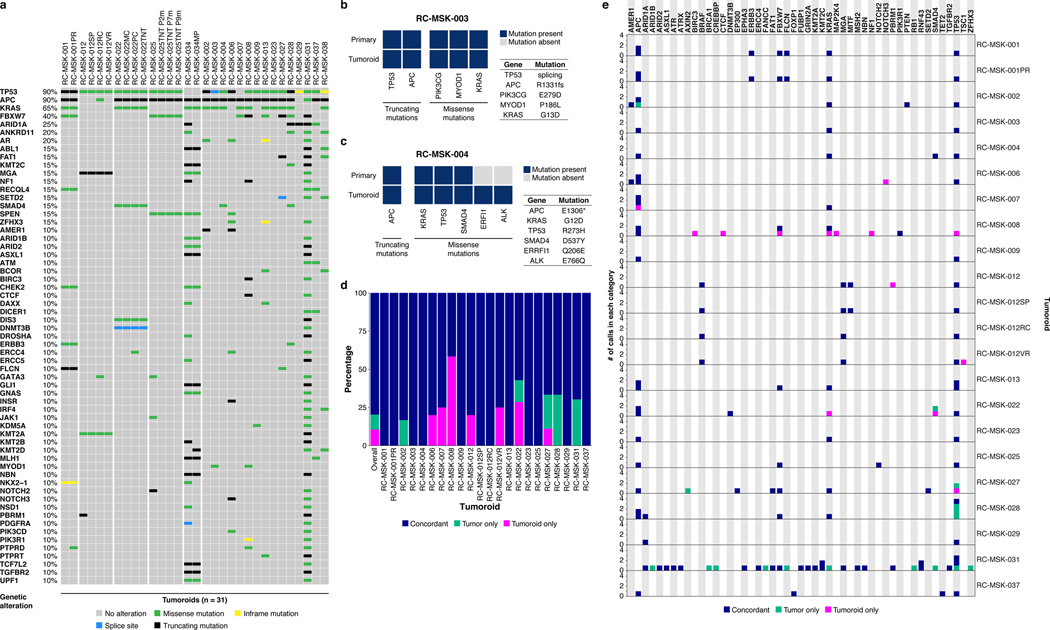
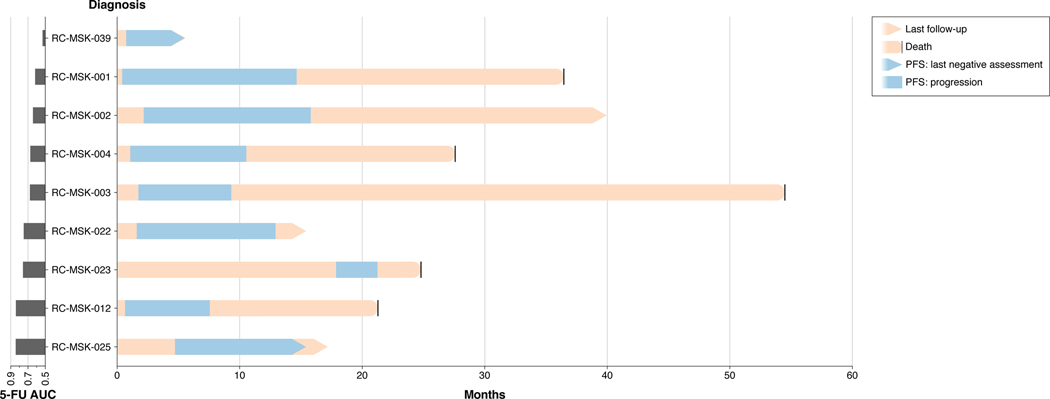
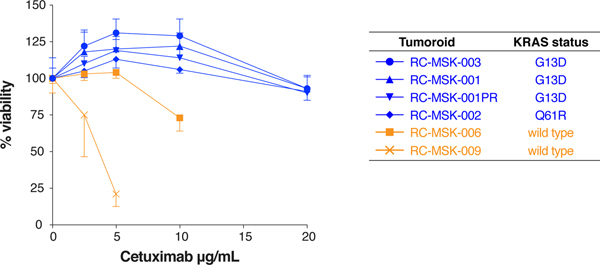
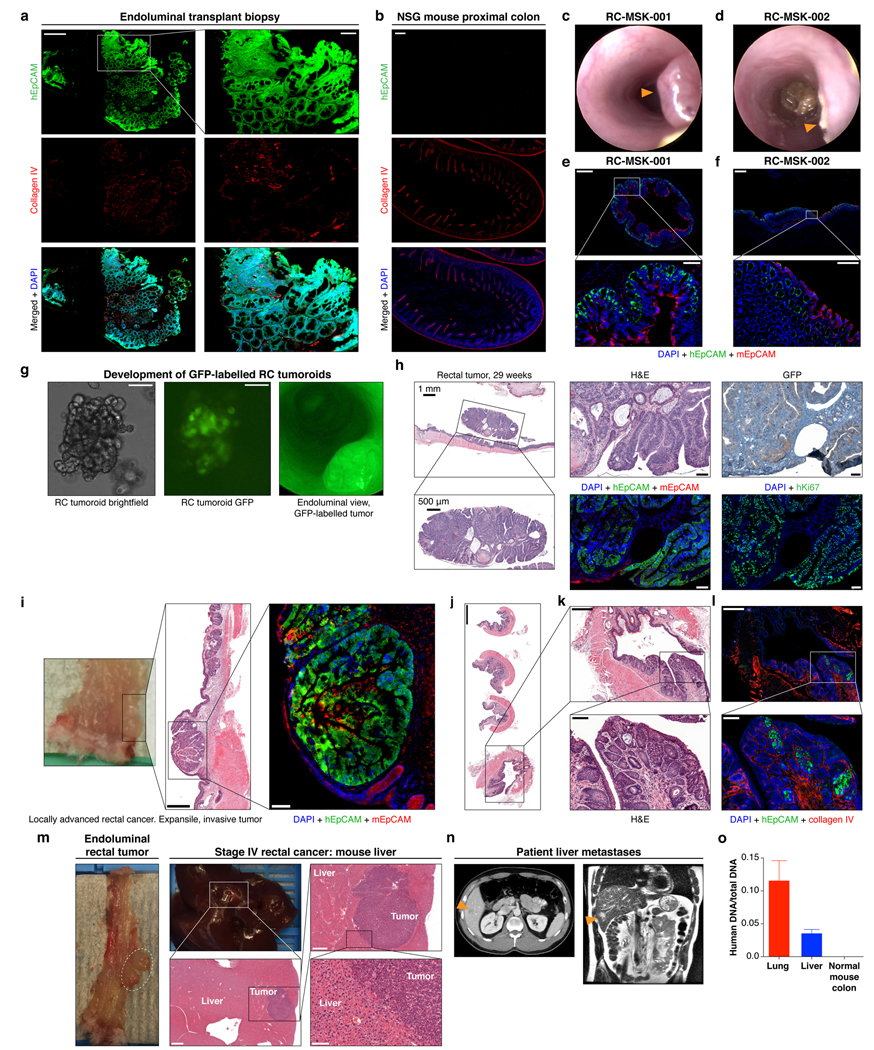
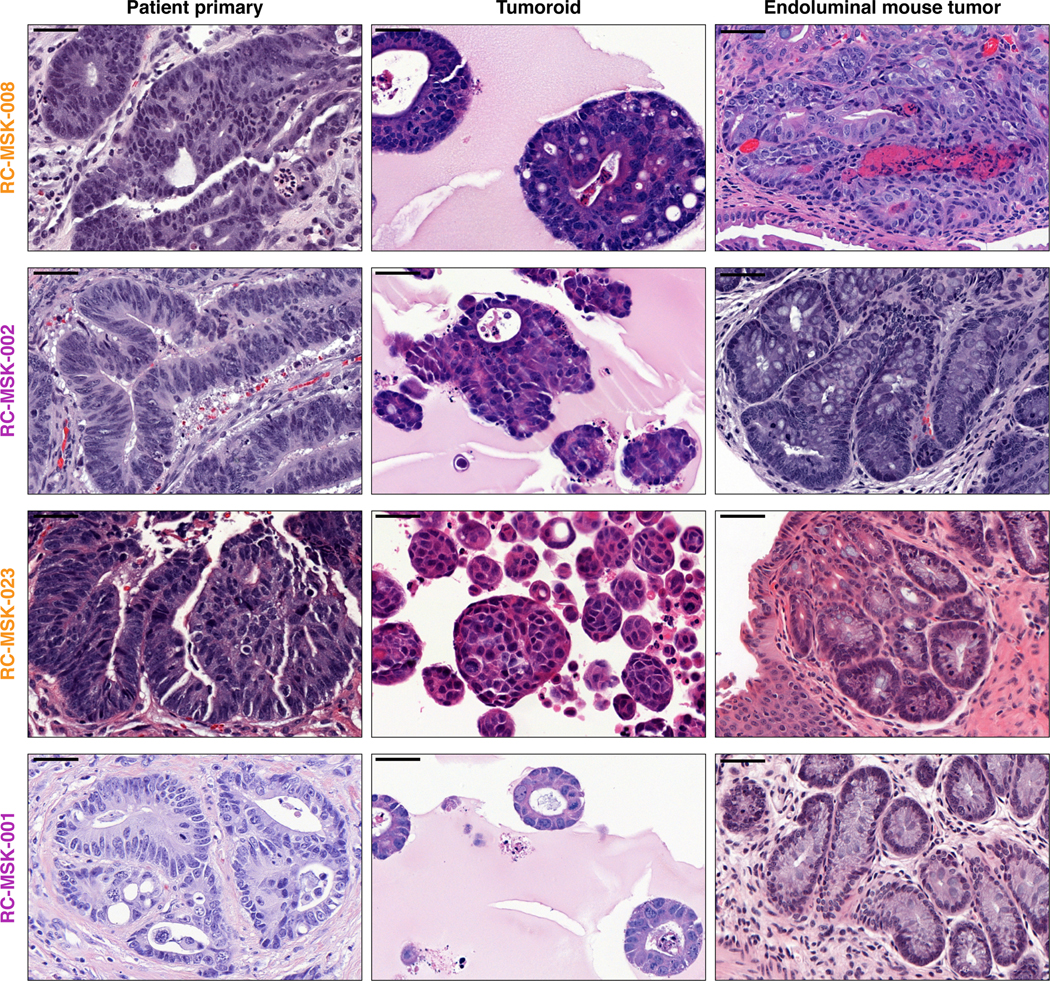
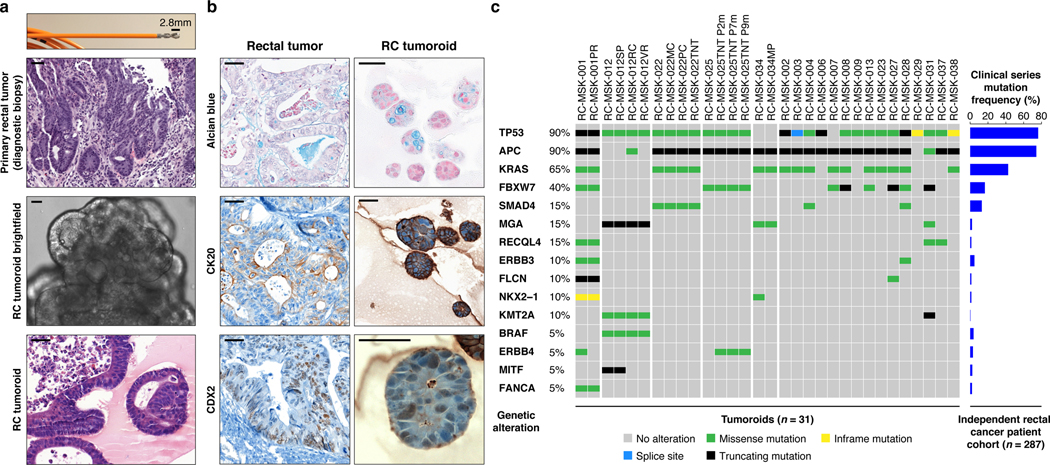
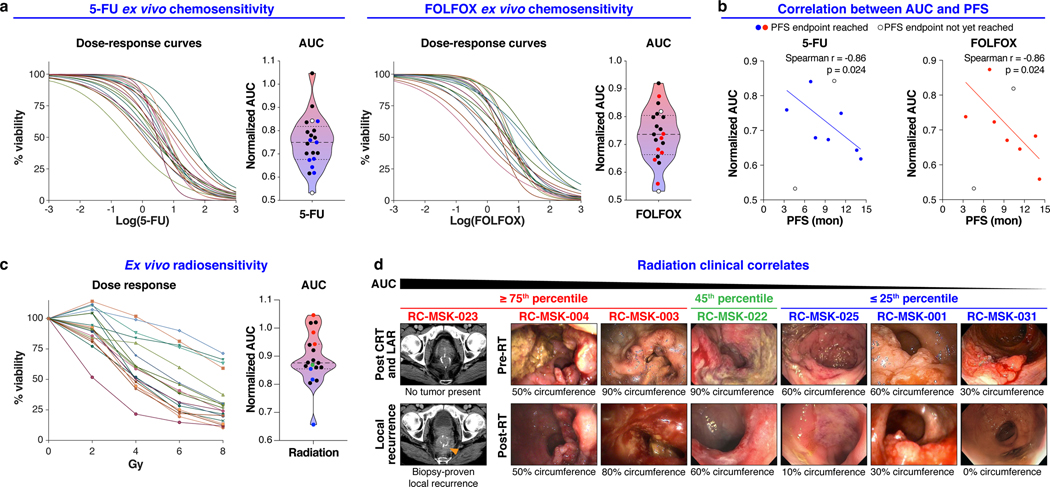
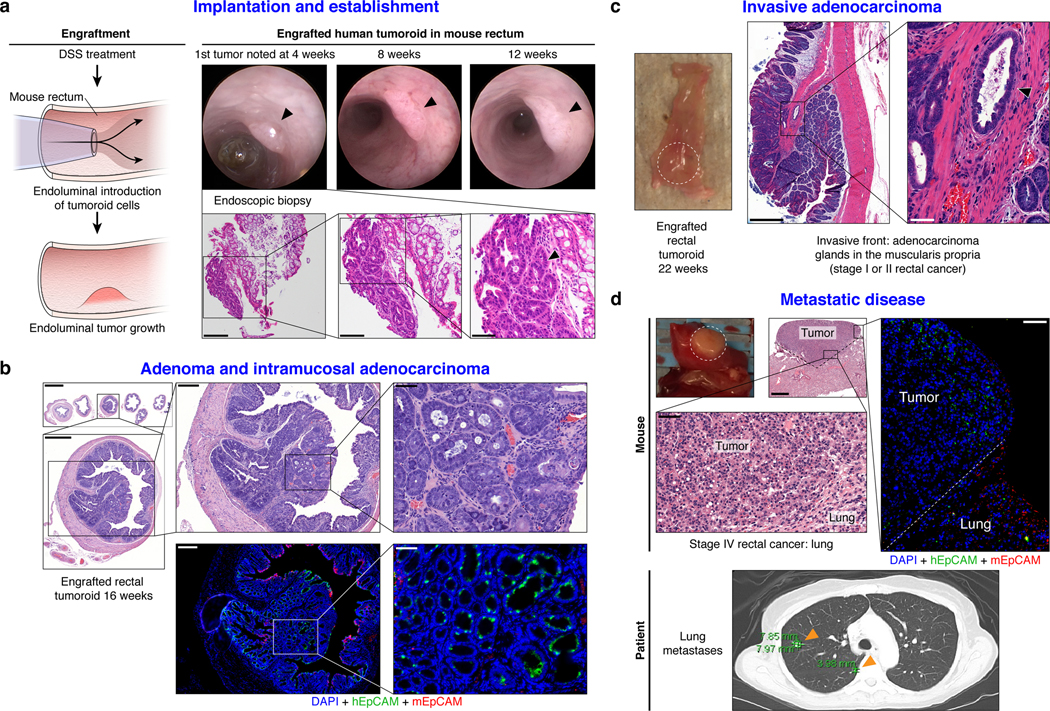
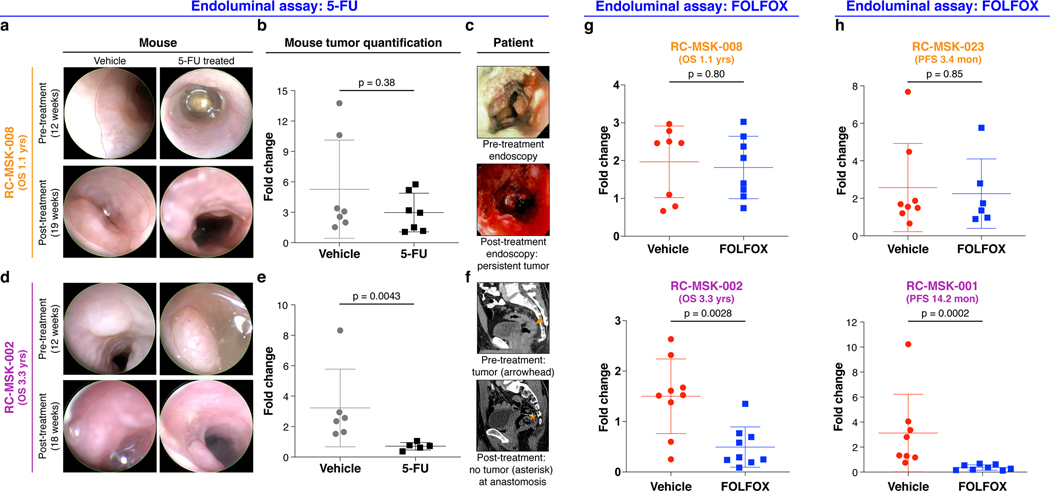
Rectal cancer (RC) is a challenging disease to treat that requires chemotherapy, radiation and surgery to optimize outcomes for individual patients. No accurate model of RC exists to answer fundamental research questions relevant to patients. We established a biorepository of 65 patient-derived RC organoid cultures (tumoroids) from patients with primary, metastatic or recurrent disease. RC tumoroids retained molecular features of the tumors from which they were derived, and their ex vivo responses to clinically relevant chemotherapy and radiation treatment correlated with the clinical responses noted in individual patients' tumors. Upon engraftment into murine rectal mucosa, human RC tumoroids gave rise to invasive RC followed by metastasis to lung and liver. Importantly, engrafted tumors displayed the heterogenous sensitivity to chemotherapy observed clinically. Thus, the biology and drug sensitivity of RC clinical isolates can be efficiently interrogated using an organoid-based, ex vivo platform coupled with in vivo endoluminal propagation in animals.
Conflict of interest statement
Competing Interests:
J.J.S. has received travel support from Intuitive Surgical Inc. and has served as a clinical advisor for Guardant Health, Inc.
C.L.S. serves on the Board of Directors of Novartis, is a co-founder of ORIC Pharm, and co-inventor of enzalutamide and apalutamide. He is a science advisor to Agios, Beigene, Blueprint, Column Group, Foghorn, Housey Pharma, Nextech, KSQ, Petra, and PMV. He was a co-founder of Seragon, purchased by Genentech/Roche in 2014.
J.M. is a science advisor and owns company stock in Scholar Rock.
H.C. is an inventor on several patents related to organoid technology.
S.W.L. is a co-founder and scientific advisory board member for ORIC Pharm, Blueprint, and Mirimus. He also serves on the scientific advisory board for Constellation, Petra, and PMV and has recently served as a consultant for Forma, Boehringer Ingelheim, and Aileron.
J.G.-A. has received support from Medtronic (honorarium for consultancy with Medtronic), Johnson & Johnson (honorarium for delivering a talk), and Intuitive Surgical (honorarium for participating in a webinar by Intuitive Surgical).
P.B.R. has received honorarium from Corning to discuss 3D cell culture techniques, has served as a consultant for AstraZeneca, and is a consultant for EMD Serono for work on radiation sensitizers.
R.N.K. is a cofounder of Ceramedix Holding L.L.C. He also has patents unrelated to this work: RK (US7195775B1, US7850984B2, and US10052387B2), RK (US8562993B2, US9592238B2, US20150216971A1, and US20170335014A1), and RK (US20170333413A1 and US20180015183A1).
K.P.O. has received an honorarium from Merck to discuss organoid platforms.
Figures
Comment in
-
Organoids as Oracles for Precision Medicine in Rectal Cancer.Cell Stem Cell. 2020 Jan 2;26(1):4-6. doi: 10.1016/j.stem.2019.12.003. Cell Stem Cell. 2020. PMID: 31951587
References
-
- Siegel RL, Miller KD & Jemal A Cancer statistics, 2019. CA. Cancer J. Clin 69, 7–34 (2019). - PubMed
-
- Deborah Freedman-Cass N et al. NCCN Guidelines Version 2.2017 Panel Members Rectal Cancer Continue NCCN Guidelines Panel Disclosures.
-
- van der Valk MJM et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet 391, 2537–2545 (2018). - PubMed
-
- Martens MH et al. Long-term Outcome of an Organ Preservation Program After Neoadjuvant Treatment for Rectal Cancer. J. Natl. Cancer Inst 108, djw171 (2016). - PubMed
Methods-only References:
-
- Sato T et al. Long-term Expansion of Epithelial Organoids From Human Colon, Adenoma, Adenocarcinoma, and Barrett’s Epithelium. Gastroenterology 141, 1762–1772 (2011). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- TL1 TR002386/TR/NCATS NIH HHS/United States
- R01 CA193837/CA/NCI NIH HHS/United States
- T32 CA009207/CA/NCI NIH HHS/United States
- K22 CA181280/CA/NCI NIH HHS/United States
- P50 CA092629/CA/NCI NIH HHS/United States
- F30 CA200110/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01 CA155169/CA/NCI NIH HHS/United States
- K08 CA230213/CA/NCI NIH HHS/United States
- P01 CA094060/CA/NCI NIH HHS/United States
- U54 CA224079/CA/NCI NIH HHS/United States
- T32 GM007739/GM/NIGMS NIH HHS/United States
- P01 CA129243/CA/NCI NIH HHS/United States
- K12 CA184746/CA/NCI NIH HHS/United States
- T32 CA160001/CA/NCI NIH HHS/United States
- U54 OD020355/OD/NIH HHS/United States
- R25 CA020449/CA/NCI NIH HHS/United States
- R01 CA182551/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
