

A luminal unfolding microneedle injector for oral delivery of macromolecules
- PMID: 31591601
- PMCID: PMC7218658
- DOI: 10.1038/s41591-019-0598-9
A luminal unfolding microneedle injector for oral delivery of macromolecules
Abstract
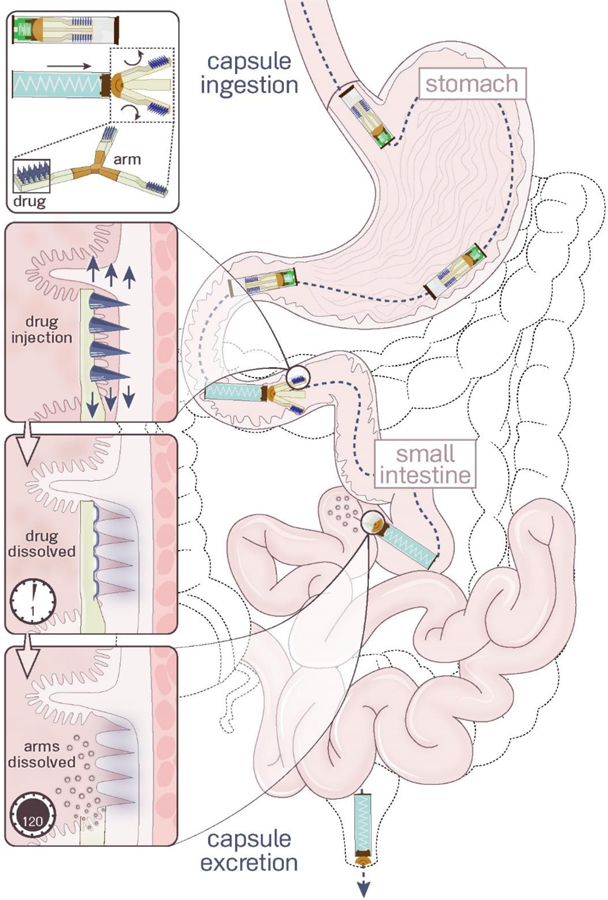
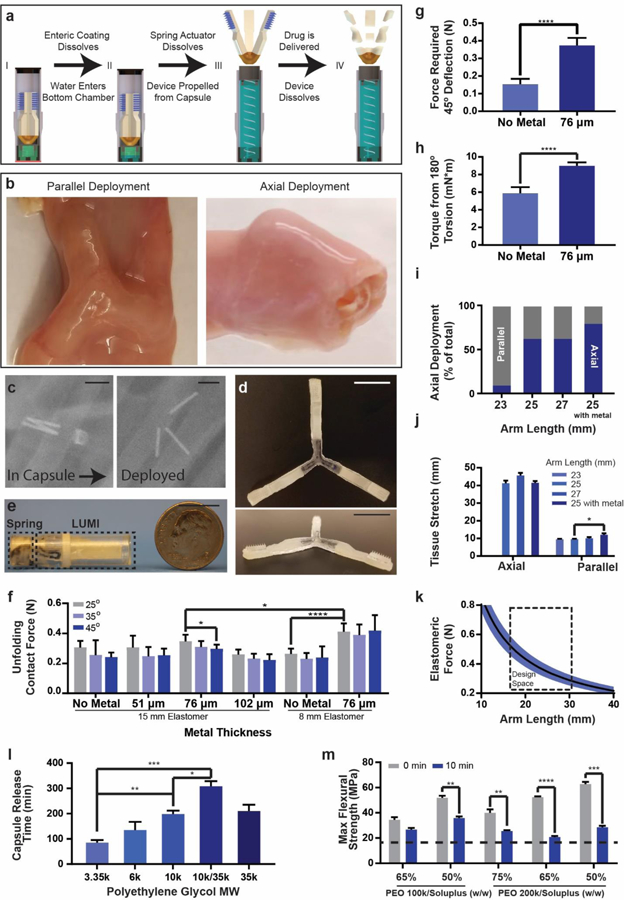
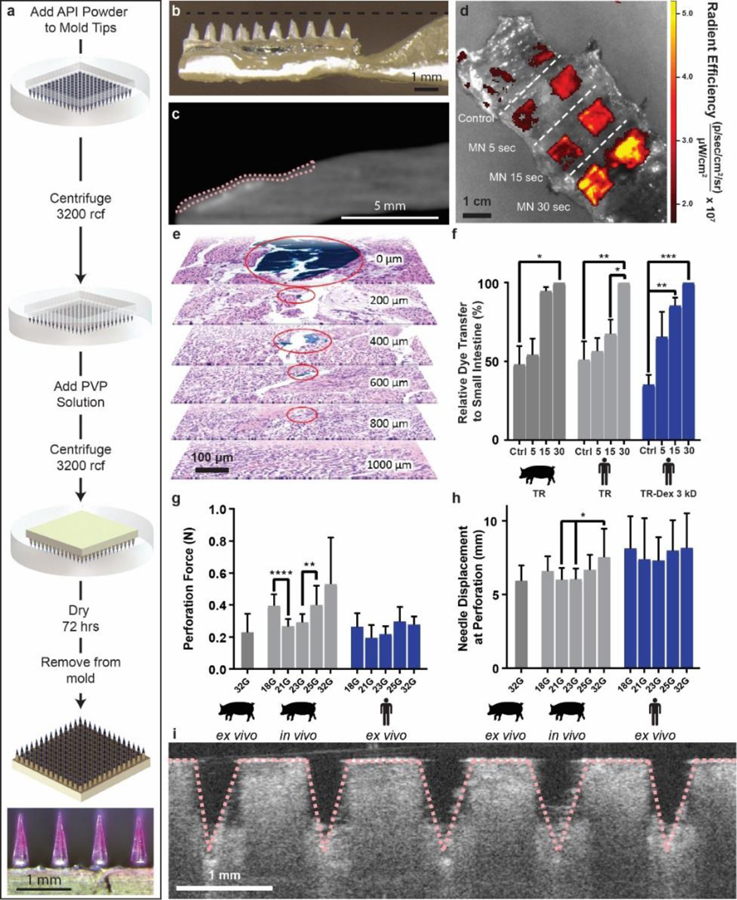
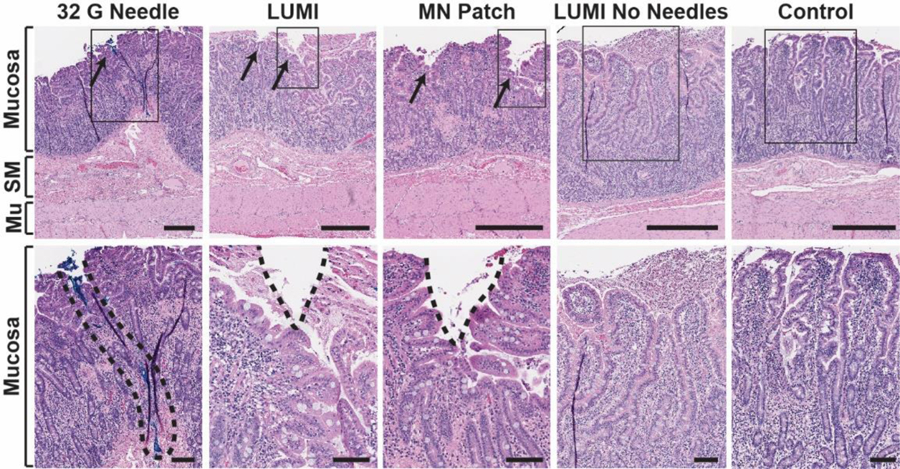
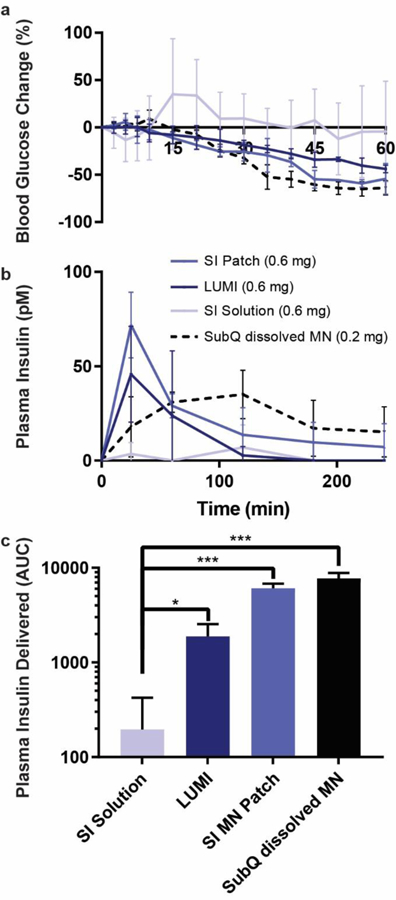
Insulin and other injectable biologic drugs have transformed the treatment of patients suffering from diabetes1,2, yet patients and healthcare providers often prefer to use and prescribe less effective orally dosed medications3-5. Compared with subcutaneously administered drugs, oral formulations create less patient discomfort4, show greater chemical stability at high temperatures6, and do not generate biohazardous needle waste7. An oral dosage form for biologic medications is ideal; however, macromolecule drugs are not readily absorbed into the bloodstream through the gastrointestinal tract8. We developed an ingestible capsule, termed the luminal unfolding microneedle injector, which allows for the oral delivery of biologic drugs by rapidly propelling dissolvable drug-loaded microneedles into intestinal tissue using a set of unfolding arms. During ex vivo human and in vivo swine studies, the device consistently delivered the microneedles to the tissue without causing complete thickness perforations. Using insulin as a model drug, we showed that, when actuated, the luminal unfolding microneedle injector provided a faster pharmacokinetic uptake profile and a systemic uptake >10% of that of a subcutaneous injection over a 4-h sampling period. With the ability to load a multitude of microneedle formulations, the device can serve as a platform to orally deliver therapeutic doses of macromolecule drugs.
Conflict of interest statement
Figures
References
-
- Korytkowski M When oral agents fail: practical barriers to starting insulin. Int. J. Obes 26, S18–S24 (2002). - PubMed
-
- Inzucchi SE et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 38, 140–9 (2015). - PubMed
-
- Matza LS et al. Utilities and disutilities for type 2 diabetes treatment-related attributes. Qual. Life Res 16, 1251–1265 (2007). - PubMed
-
- Boye KS et al. Utilities and disutilities for attributes of injectable treatments for type 2 diabetes. Eur. J. Heal. Econ 12, 219–230 (2011). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
