

Glycine receptor autoantibodies disrupt inhibitory neurotransmission
- PMID: 31591639
- PMCID: PMC6821286
- DOI: 10.1093/brain/awz297
Glycine receptor autoantibodies disrupt inhibitory neurotransmission
Abstract
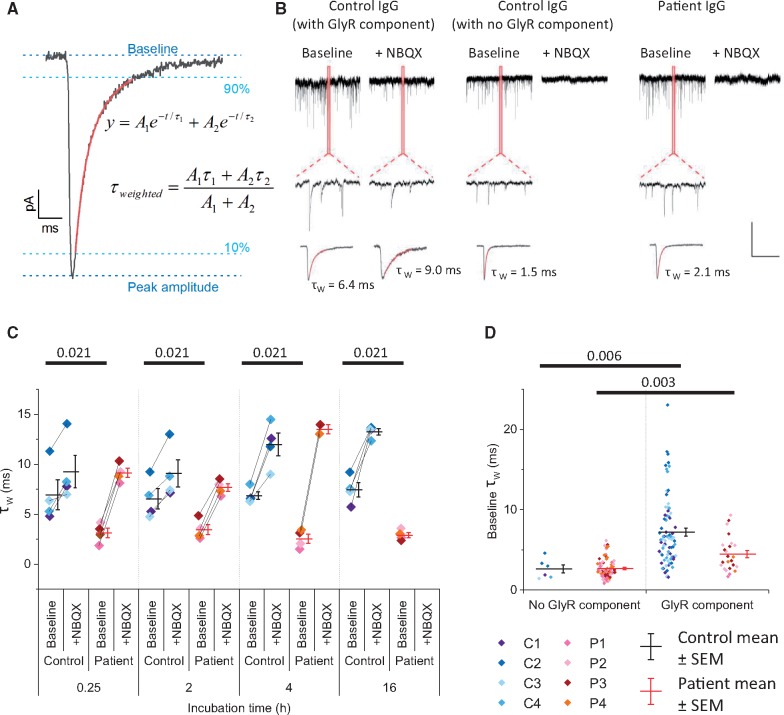
Chloride-permeable glycine receptors have an important role in fast inhibitory neurotransmission in the spinal cord and brainstem. Human immunoglobulin G (IgG) autoantibodies to glycine receptors are found in a substantial proportion of patients with progressive encephalomyelitis with rigidity and myoclonus, and less frequently in other variants of stiff person syndrome. Demonstrating a pathogenic role of glycine receptor autoantibodies would help justify the use of immunomodulatory therapies and provide insight into the mechanisms involved. Here, purified IgGs from four patients with progressive encephalomyelitis with rigidity and myoclonus or stiff person syndrome, and glycine receptor autoantibodies, were observed to disrupt profoundly glycinergic neurotransmission. In whole-cell patch clamp recordings from cultured rat spinal motor neurons, glycinergic synaptic currents were almost completely abolished following incubation in patient IgGs. Most human autoantibodies targeting other CNS neurotransmitter receptors, such as N-methyl-d-aspartate (NMDA) receptors, affect whole cell currents only after several hours incubation and this effect has been shown to be the result of antibody-mediated crosslinking and internalization of receptors. By contrast, we observed substantial reductions in glycinergic currents with all four patient IgG preparations with 15 min of exposure to patient IgGs. Moreover, monovalent Fab fragments generated from the purified IgG of three of four patients also profoundly reduced glycinergic currents compared with control Fab-IgG. We conclude that human glycine receptor autoantibodies disrupt glycinergic neurotransmission, and also suggest that the pathogenic mechanisms include direct antagonistic actions on glycine receptors.
Keywords: autoantibody; glycine receptor; progressive encephalomyelitis with rigidity and myoclonus (PERM); stiff person syndrome (SPS).
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures



References
-
- Brenner T, Sills GJ, Hart Y, Howell S, Waters P, Brodie MJ, et al.Prevalence of neurologic autoantibodies in cohorts of patients with new and established epilepsy. Epilepsia 2013; 54: 1028–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- G0900613/MRC_/Medical Research Council/United Kingdom
- G0400136/MRC_/Medical Research Council/United Kingdom
- G0801316/MRC_/Medical Research Council/United Kingdom
- G0600368/MRC_/Medical Research Council/United Kingdom
- G0601440/MRC_/Medical Research Council/United Kingdom
- G116/147/MRC_/Medical Research Council/United Kingdom
- G0400627/MRC_/Medical Research Council/United Kingdom
- G9805989/MRC_/Medical Research Council/United Kingdom
- MR/L01095X/1/MRC_/Medical Research Council/United Kingdom
- 209807/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- 212285/Z/18/Z/WT_/Wellcome Trust/United Kingdom
