

Physiological effects of high-flow oxygen in tracheostomized patients
- PMID: 31591659
- PMCID: PMC6779681
- DOI: 10.1186/s13613-019-0591-y
Physiological effects of high-flow oxygen in tracheostomized patients
Abstract
Background: High-flow oxygen therapy via nasal cannula (HFOTNASAL) increases airway pressure, ameliorates oxygenation and reduces work of breathing. High-flow oxygen can be delivered through tracheostomy (HFOTTRACHEAL), but its physiological effects have not been systematically described. We conducted a cross-over study to elucidate the effects of increasing flow rates of HFOTTRACHEAL on gas exchange, respiratory rate and endotracheal pressure and to compare lower airway pressure produced by HFOTNASAL and HFOTTRACHEAL. METHODS: Twenty-six tracheostomized patients underwent standard oxygen therapy through a conventional heat and moisture exchanger, and then HFOTTRACHEAL through a heated humidifier, with gas flow set at 10, 30 and 50 L/min. Each step lasted 30 min; gas flow sequence during HFOTTRACHEAL was randomized. In five patients, measurements were repeated during HFOTTRACHEAL before tracheostomy decannulation and immediately after during HFOTNASAL. In each step, arterial blood gases, respiratory rate, and tracheal pressure were measured.
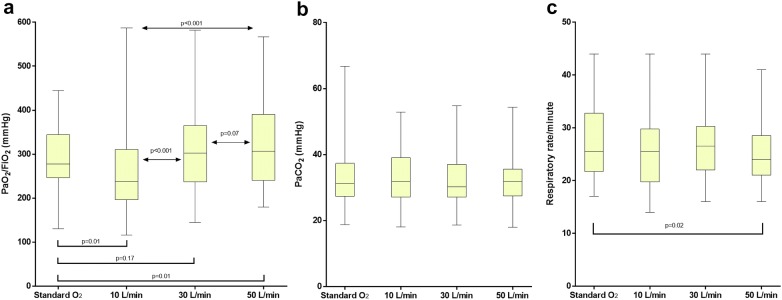
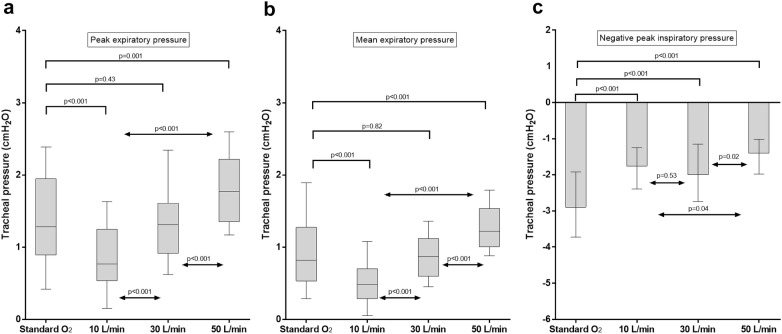
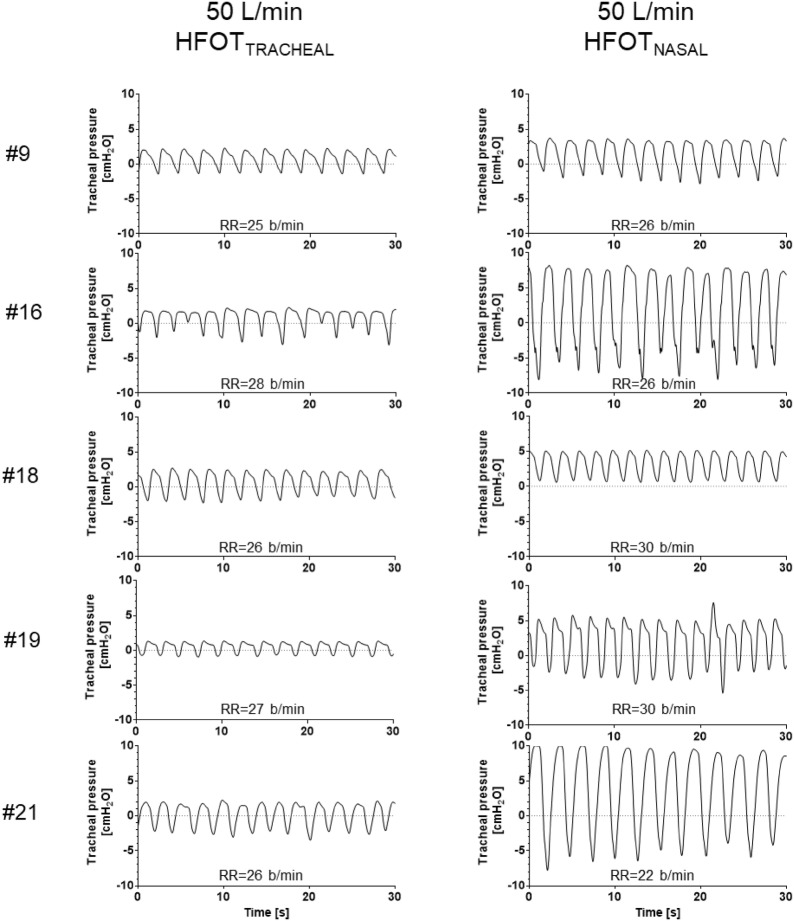
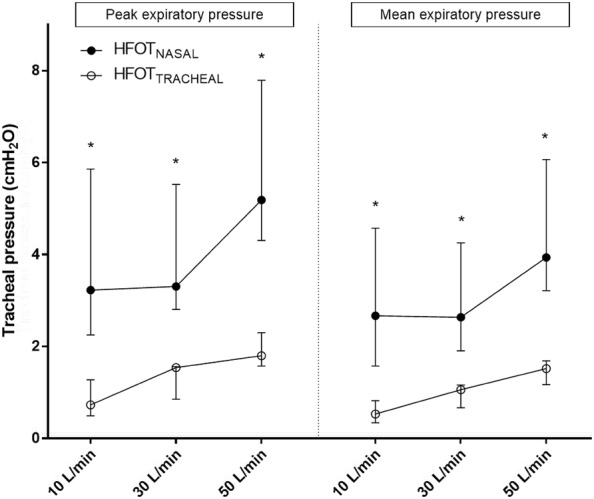
Results: During HFOTTRACHEAL, PaO2/FiO2 ratio and tracheal expiratory pressure slightly increased proportionally to gas flow. The mean [95% confidence interval] expiratory pressure raise induced by 10-L/min increase in flow was 0.2 [0.1-0.2] cmH2O (ρ = 0.77, p < 0.001). Compared to standard oxygen, HFOTTRACHEAL limited the negative inspiratory swing in tracheal pressure; at 50 L/min, but not with other settings, HFOTTRACHEAL increased mean tracheal expiratory pressure by (mean difference [95% CI]) 0.4 [0.3-0.6] cmH2O, peak tracheal expiratory pressure by 0.4 [0.2-0.6] cmH2O, improved PaO2/FiO2 ratio by 40 [8-71] mmHg, and reduced respiratory rate by 1.9 [0.3-3.6] breaths/min without PaCO2 changes. As compared to HFOTTRACHEAL, HFOTNASAL produced higher tracheal mean and peak expiratory pressure (at 50 L/min, mean difference [95% CI]: 3 [1-5] cmH2O and 4 [1-7] cmH2O, respectively).
Conclusions: As compared to standard oxygen, 50 L/min of HFOTTRACHEAL are needed to improve oxygenation, reduce respiratory rate and provide small degree of positive airway expiratory pressure, which, however, is significantly lower than the one produced by HFOTNASAL.
Keywords: Mechanical ventilator weaning; Oxygen inhalation therapy; Positive end-expiratory pressure; Respiratory insufficiency; Tracheostomy.
Conflict of interest statement
DLG has received payments for travel expenses by Maquet, Getinge and Air Liquide. MA has received payments for Board participation from Maquet, Air Liquide and Chiesi. DLG and MA disclose a research grant by General Electric Healthcare. SMM is the principal investigator of the RINO trial (clinicaltrials.gov, NCT02107183), which was supported by Fisher and Paykel healthcare.
Figures
References
-
- Roca O, Hernández G, Díaz-Lobato S, Carratalá JM, Gutiérrez RM, Masclans JR, et al. Current evidence for the effectiveness of heated and humidified high flow nasal cannula supportive therapy in adult patients with respiratory failure. Crit Care. 2016;20:109. doi: 10.1186/s13054-016-1263-z. - DOI - PMC - PubMed
-
- Frat J-P, Ragot S, Girault C, Perbet S, Prat G, Boulain T, et al. Effect of non-invasive oxygenation strategies in immunocompromised patients with severe acute respiratory failure: a post hoc analysis of a randomised trial. Lancet Respir Med. 2016;4:646–652. doi: 10.1016/S2213-2600(16)30093-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
