

Injectable Tissue Replacement and Regeneration: Anatomic Fat Grafting to Restore Decayed Facial Tissues
- PMID: 31592023
- PMCID: PMC6756675
- DOI: 10.1097/GOX.0000000000002293
Injectable Tissue Replacement and Regeneration: Anatomic Fat Grafting to Restore Decayed Facial Tissues
Abstract
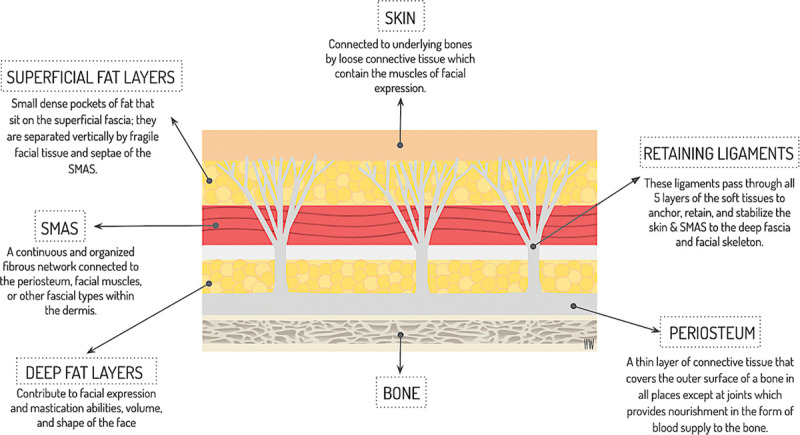
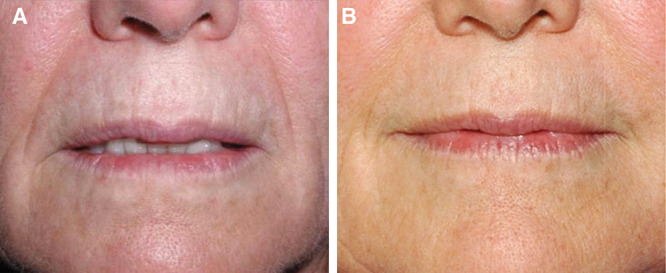
Aging is a dynamic process that can be modeled and understood tissue by tissue and cell by cell. Numerous authors have helped us understand the anatomy of facial fat compartments and the effects of aging on our facial tissues such as skin, fat, bone and fibrous ligaments. Injectable tissue replacement and regeneration (ITR2) is a method to replace decayed tissues of the face using "like tissues" in an effort to delay or slow the rate of tissue decay seen in facial aging. Facial topography and proportion analysis are performed to diagnose individual-specific losses of facial fat. The degree of sun damage and skin thinning is noted as is the degree of loss in the superficial fat compartment. Deep compartment fat loss is evaluated as is pyriform aperture, orbital, mandibular ramus, mandibular body, and chin resorption. From this analysis, a detailed treatment plan is formulated. Using a mechanical device, 3 different fat grafts are created: 2 mm (millifat), 1 mm (microfat), and 500 microns (cell optimized, matrix rich nanofat); anatomic replacement of all areas of tissue loss is carried out. Millifat is used for deep compartment and bone losses, microfat for superficial fat losses above the facial musculature and nanofat is used intradermally and as a biological cream for topical application. The rationale behind this standardized approach is explained and the scientific foundations for the idea are presented. Reduction in tissue decay appears to be a valid observation, but awaits others confirmation.
Copyright © 2019 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Figures








Similar articles
-
Fat Grafting for Facial Rejuvenation through Injectable Tissue Replacement and Regeneration: A Differential, Standardized, Anatomic Approach.Clin Plast Surg. 2020 Jan;47(1):31-41. doi: 10.1016/j.cps.2019.08.005. Epub 2019 Oct 28. Clin Plast Surg. 2020. PMID: 31739895 Review.
-
Regenerative Cells For Facial Surgery: Biofilling and Biocontouring.Aesthet Surg J. 2017 Jul 1;37(suppl_3):S16-S32. doi: 10.1093/asj/sjx078. Aesthet Surg J. 2017. PMID: 29025218 Review.
-
Standardized Anatomic and Regenerative Facial Fat Grafting: Objective Photometric Evaluation 1 to 19 Months After Injectable Tissue Replacement and Regeneration.Aesthet Surg J. 2022 Mar 15;42(4):327-339. doi: 10.1093/asj/sjab379. Aesthet Surg J. 2022. PMID: 34724035
-
Fat transplant: Amazing growth and regeneration of cells and rebirth with the miracle of fat cells.J Cosmet Dermatol. 2024 Apr;23(4):1141-1149. doi: 10.1111/jocd.16103. Epub 2023 Nov 27. J Cosmet Dermatol. 2024. PMID: 38010992 Review.
-
Microfat and Nanofat: When and Where These Treatments Work.Facial Plast Surg Clin North Am. 2019 Aug;27(3):321-330. doi: 10.1016/j.fsc.2019.03.004. Facial Plast Surg Clin North Am. 2019. PMID: 31280846 Review.
Cited by
-
New Mechanical Fat Separation Technique: Adjustable Regenerative Adipose-tissue Transfer (ARAT) and Mechanical Stromal Cell Transfer (MEST).Aesthet Surg J Open Forum. 2020 Jul 22;2(4):ojaa035. doi: 10.1093/asjof/ojaa035. eCollection 2020 Dec. Aesthet Surg J Open Forum. 2020. PMID: 33791661 Free PMC article.
-
Translational products of adipose tissue-derived mesenchymal stem cells: Bench to bedside applications.World J Stem Cells. 2021 Oct 26;13(10):1360-1381. doi: 10.4252/wjsc.v13.i10.1360. World J Stem Cells. 2021. PMID: 34786149 Free PMC article. Review.
-
Not Stromal Vascular Fraction (SVF) or Nanofat, but Total Stromal-Cells (TOST): A New Definition. Systemic Review of Mechanical Stromal-Cell Extraction Techniques.Tissue Eng Regen Med. 2021 Feb;18(1):25-36. doi: 10.1007/s13770-020-00313-0. Epub 2020 Nov 24. Tissue Eng Regen Med. 2021. PMID: 33231864 Free PMC article.
-
Indication-based protocols with different solutions for mechanical stromal-cell transfer.Scars Burn Heal. 2022 Jan 5;8:20595131211047830. doi: 10.1177/20595131211047830. eCollection 2022 Jan-Dec. Scars Burn Heal. 2022. PMID: 35003762 Free PMC article.
References
-
- Lambros V. Observations on periorbital and midface aging. Plast Reconstr Surg. 2007;120:1367–1376; discussion 1377. - PubMed
-
- Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227; discussion 2228. - PubMed
-
- Kahn DM, Shaw RB, Jr. Aging of the bony orbit: a three-dimensional computed tomographic study. Aesthet Surg J. 2008;28:258–264. - PubMed
LinkOut - more resources
Full Text Sources