

Nationwide in-hospital mortality following colonic cancer resection according to hospital volume in Germany
- PMID: 31592096
- PMCID: PMC6773649
- DOI: 10.1002/bjs5.50173
Nationwide in-hospital mortality following colonic cancer resection according to hospital volume in Germany
Abstract
Background: Colonic cancer is the most common cancer of the gastrointestinal tract. The aim of this study was to determine mortality rates following colonic cancer resection and the effect of hospital caseload on in-hospital mortality in Germany.
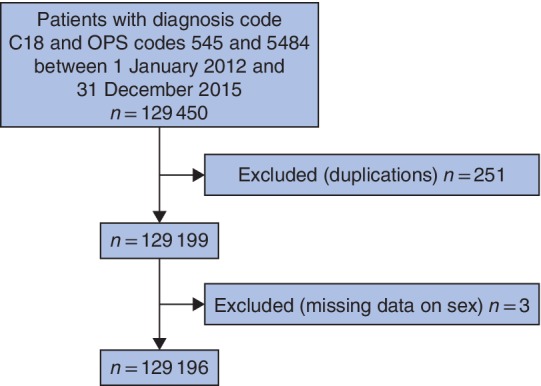
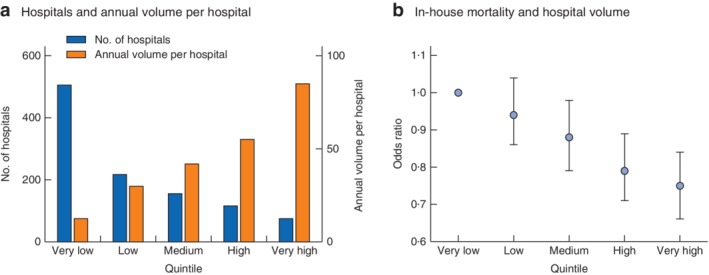
Methods: Patients admitted with a diagnosis of colonic cancer undergoing colonic resection from 2012 to 2015 were identified from a nationwide registry using procedure codes. The outcome measure was in-hospital mortality. Hospitals were ranked according to their caseload for colonic cancer resection, and patients were categorized into five subgroups on the basis of hospital volume.
Results: Some 129 196 colonic cancer resections were reviewed. The overall in-house mortality rate was 5·8 per cent, ranging from 6·9 per cent (1775 of 25 657 patients) in very low-volume hospitals to 4·8 per cent (1239 of 25 825) in very high-volume centres (P < 0·001). In multivariable logistic regression analysis the risk-adjusted odds ratio for in-house mortality was 0·75 (95 per cent c.i. 0·66 to 0·84) in very high-volume hospitals performing a mean of 85·0 interventions per year, compared with that in very low-volume hospitals performing a mean of only 12·7 interventions annually, after adjustment for sex, age, co-morbidity, emergency procedures, prolonged mechanical ventilation and transfusion.
Conclusion: In Germany, patients undergoing colonic cancer resections in high-volume hospitals had with improved outcomes compared with patients treated in low-volume hospitals.
Antecedentes: El cáncer de colon es el cáncer más frecuente del tracto digestivo. El objetivo de este estudio fue determinar las tasas de mortalidad tras resección de cáncer de colon y el efecto del volumen de casos del hospital sobre la mortalidad intrahospitalaria en Alemania.
Métodos: Los pacientes ingresados con el diagnóstico de cáncer de colon sometidos a resección colónica entre 2012 y 2015 se identificaron a partir de un registro nacional utilizando los códigos de los procedimientos. La medida de resultado fue la mortalidad intrahospitalaria. Los hospitales se clasificaron de acuerdo con su número de casos de resecciones de cáncer de colon y los pacientes fueron categorizados en 5 diferentes subgrupos en la base del volumen del hospital.
Resultados: Se revisaron 129.196 resecciones de cáncer de colon. La tasa de mortalidad fue de 5,75%, variando desde 6,92% (n = 1.775) en hospitales de bajo volumen hasta 4,80% (n = 1.239) en centros con alto volumen, con una diferencia significativa entre los escenarios de bajo y alto volumen (P < 0,001). El análisis de regresión logística multivariable puso de manifiesto que la razón de oportunidades (odds ratio, OR) ajustada al riesgo de la mortalidad intrahospitalaria fue de 0,75 (i.c. del 95% 0,66‐0,84) en hospitales con volumen muy alto que realizaban más de 85,0 intervenciones/año, en comparación con hospitales de volumen muy bajo que realizaban menos de 13 intervenciones/año, tras ajustar por sexo, edad, comorbilidad, procedimiento urgente, ventilación mecánica prolongada y transfusiones.
Conclusión: En Alemania, los pacientes sometidos a resección de cáncer de colon en hospitales de alto volumen tienen mejores resultados en comparación con los pacientes tratados en centros de bajo volumen.
In Germany, perioperative mortality for colonic cancer resection at the national level is high. Patients undergoing resection of colonic cancer in high‐volume hospitals have improved outcomes compared with those treated in low‐volume hospitals. Mortality rate, hospital volume and CRC resections.
© 2019 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, Barzi A et al. Colorectal cancer statistics, 2017. CA Cancer J Clin 2017; 67: 177–193. - PubMed
-
- André T, Boni C, Mounedji‐Boudiaf L, Navarro M, Tabernero J, Hickish T et al.; Multicenter International Study of Oxaliplatin/5‐Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) Investigators. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004; 350: 2343–2351. - PubMed
-
- André T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 2009; 27: 3109–3116. - PubMed
-
- André T, de Gramont A, Vernerey D, Chibaudel B, Bonnetain F, Tijeras‐Raballand A et al. Adjuvant fluorouracil, leucovorin, and oxaliplatin in stage II to III colon cancer: updated 10‐year survival and outcomes according to BRAF mutation and mismatch repair status of the MOSAIC study. J Clin Oncol 2015; 33: 4176–4187. - PubMed
-
- Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation – technical notes and outcome. Colorectal Dis 2009; 11: 354–364. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
