

Effect of a Hospital-Initiated Program Combining Transitional Care and Long-term Self-management Support on Outcomes of Patients Hospitalized With Chronic Obstructive Pulmonary Disease: A Randomized Clinical Trial
- PMID: 31593271
- PMCID: PMC6784754
- DOI: 10.1001/jama.2019.11982
Effect of a Hospital-Initiated Program Combining Transitional Care and Long-term Self-management Support on Outcomes of Patients Hospitalized With Chronic Obstructive Pulmonary Disease: A Randomized Clinical Trial
Abstract
Importance: Patients hospitalized for chronic obstructive pulmonary disease (COPD) exacerbations have high rehospitalization rates and reduced quality of life.
Objective: To evaluate whether a hospital-initiated program that combined transition and long-term self-management support for patients hospitalized due to COPD and their family caregivers can improve outcomes.
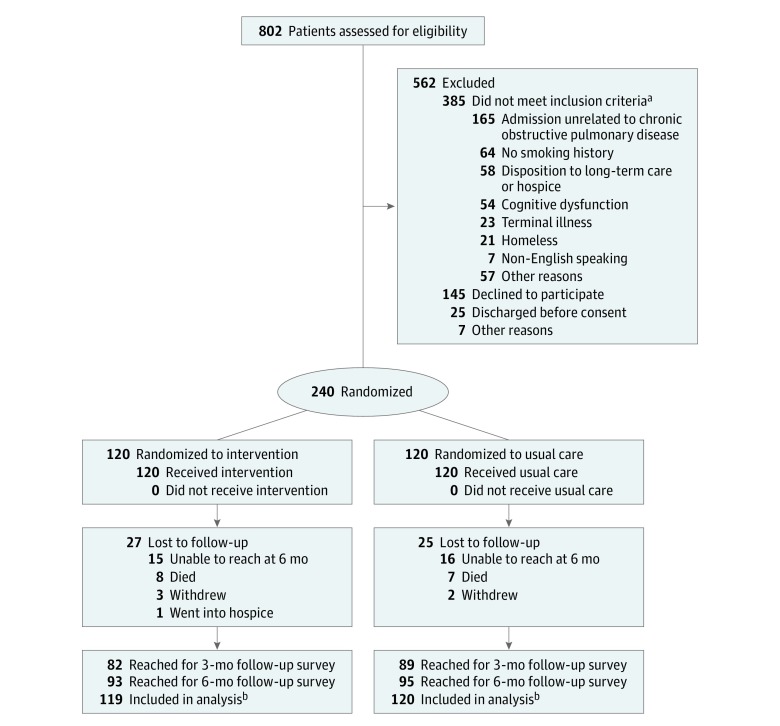
Design, setting, and participants: Single-site randomized clinical trial conducted in Baltimore, Maryland, with 240 participants. Participants were patients hospitalized due to COPD, randomized to intervention or usual care, and followed up for 6 months after hospital discharge. Enrollment occurred from March 2015 to May 2016; follow-up ended in December 2016.
Interventions: The intervention (n = 120) involved a comprehensive 3-month program to help patients and their family caregivers with long-term self-management of COPD. It was delivered by nurses with special training on supporting patients with COPD using standardized tools. Usual care (n = 120) included transition support for 30 days after discharge to ensure adherence to discharge plan and connection to outpatient care.
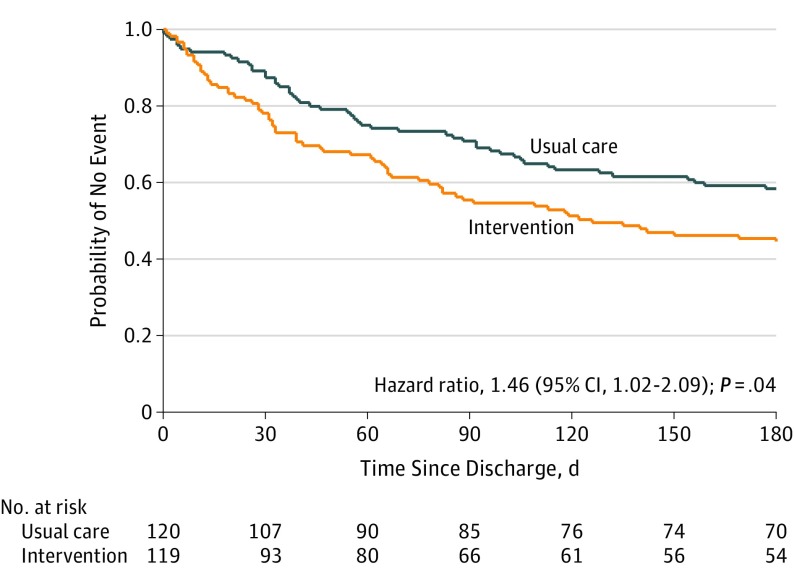
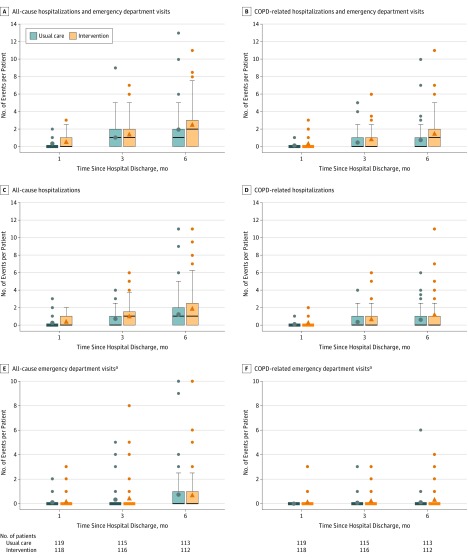
Main outcomes and measures: The primary outcome was number of COPD-related acute care events (hospitalizations and emergency department visits) per participant at 6 months. The co-primary outcome was change in participants' health-related quality of life measured by the St George's Respiratory Questionnaire (SGRQ) at 6 months after discharge (score, 0 [best] to 100 [worst]; 4-point difference is clinically meaningful).
Results: Among 240 patients who were randomized (mean [SD] age, 64.9 [9.8] years; 61.7% women), 203 (85%) completed the study. The mean (SD) baseline SGRQ score was 62.3 (18.8) in the intervention group and 63.6 (17.4) in the usual care group. The mean number of COPD-related acute care events per participant at 6 months was 1.40 (95% CI, 1.01-1.79) in the intervention group vs 0.72 (95% CI, 0.45-0.97) in the usual care group (difference, 0.68 [95% CI, 0.22-1.15]; P = .004). The mean change in participants' SGRQ total score at 6 months was 2.81 in the intervention group and -2.69 in the usual care group (adjusted difference, 5.18 [95% CI, -2.15 to 12.51]; P = .11). During the study period, there were 15 deaths (intervention: 8; usual care: 7) and 339 hospitalizations (intervention: 202; usual care: 137).
Conclusions and relevance: In a single-site randomized clinical trial of patients hospitalized due to COPD, a 3-month program that combined transition and long-term self-management support resulted in significantly greater COPD-related hospitalizations and emergency department visits, without improvement in quality of life. Further research is needed to determine reasons for this unanticipated finding.
Trial registration: ClinicalTrials.gov Identifier: NCT02036294.
Conflict of interest statement
Figures
Retracted and republished from
-
Ensuring an Accurate Scientific Record-Retraction and Republication.JAMA. 2019 Oct 8;322(14):1380. doi: 10.1001/jama.2019.14503. JAMA. 2019. Retracted and republished in: JAMA. 2019 Oct 8;322(14):1357-1359. doi: 10.1001/jama.2019.12976. Retracted and republished in: JAMA. 2019 Oct 8;322(14):1371-1380. doi: 10.1001/jama.2019.11982. PMID: 31593257 Retracted and republished. No abstract available.
Comment in
-
Unexpected Harm From an Intensive COPD Intervention.JAMA. 2019 Oct 8;322(14):1357-1359. doi: 10.1001/jama.2019.12976. JAMA. 2019. PMID: 31593255 No abstract available.
-
Critically appraised paper: In people hospitalised with chronic obstructive pulmonary disease, a combined transition and self-management program increased healthcare utilisation [synopsis].J Physiother. 2020 Apr;66(2):128. doi: 10.1016/j.jphys.2020.02.003. Epub 2020 Apr 11. J Physiother. 2020. PMID: 32291220 No abstract available.
-
Critically appraised paper: In people hospitalised with chronic obstructive pulmonary disease, a combined transition and self-management program increased healthcare utilisation [commentary].J Physiother. 2020 Apr;66(2):128. doi: 10.1016/j.jphys.2020.02.002. Epub 2020 Apr 11. J Physiother. 2020. PMID: 32291221 No abstract available.
References
-
- Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2016: NCHS Data Brief, No. 293. Hyattsville, MD: National Center for Health Statistics; 2017. - PubMed
-
- Brault MW, Hootman J, Helmick CG, Theis KA, Armour BS; Centers for Disease Control and Prevention (CDC) . Prevalence and most common causes of disability among adults: United States, 2005. MMWR Morb Mortal Wkly Rep. 2009;58(16):421-426. - PubMed
