

Home Virtual Visits for Outpatient Follow-Up Stroke Care: Cross-Sectional Study
- PMID: 31593536
- PMCID: PMC6803894
- DOI: 10.2196/13734
Home Virtual Visits for Outpatient Follow-Up Stroke Care: Cross-Sectional Study
Abstract
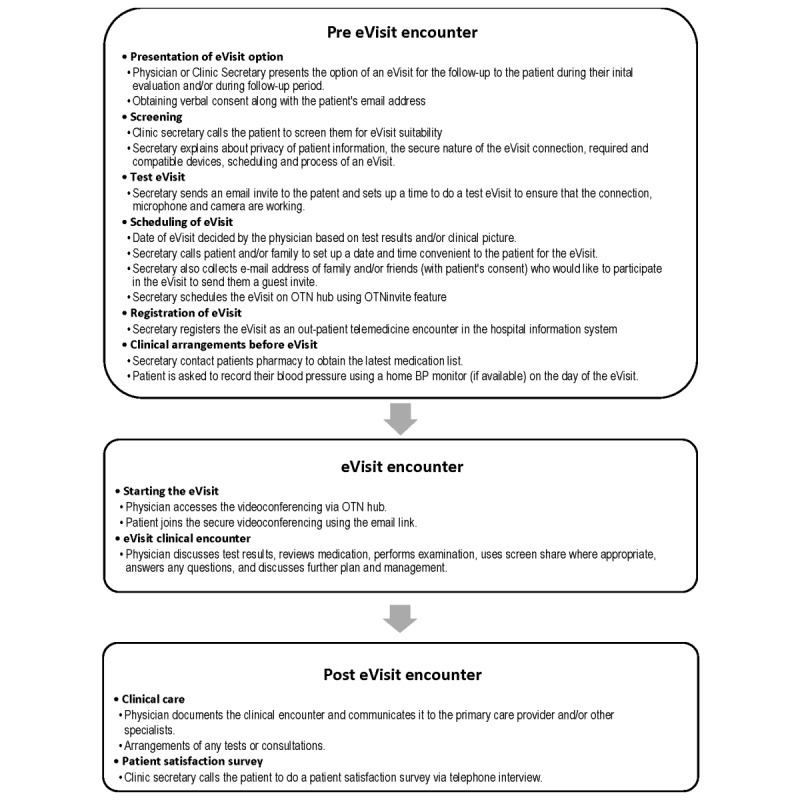
Background: Timely, in-person access to health care is a challenge for people living with conditions such as stroke that result in frailty, loss of independence, restrictions in driving and mobility, and physical and cognitive decline. In Southeastern Ontario, access is further complicated by rurality and the long travel distances to visit physician clinics. There is a need to make health care more accessible and convenient. Home virtual visits (electronic visits, eVisits) can conveniently connect physicians to patients. Physicians use a secure personal videoconferencing tool to connect to patients in their homes. Patients use their device of choice (smartphone, tablet, laptop, or desktop) for the visit.
Objective: This study aimed to assess the feasibility and logistics of implementing eVisits in a stroke prevention clinic for seniors.
Methods: A 6-month eVisit pilot study was initiated in the Kingston Health Sciences Centre stroke prevention clinic in August 2018. eVisits were used only for follow-up patient encounters. An integrated evaluation was used to test the impact of the program on clinic workflow and patient satisfaction. Patient satisfaction was evaluated by telephone interviews, using a brief questionnaire. Access and patient satisfaction metrics were compared with concurrent standard of care (patients' prior personal experience with in-person visits). Values are presented as median (interquartile range).
Results: There were 75 subjects in the pilot. The patients were aged 65 (56-73.5) years, and 39% (29/75) resided in rural areas. There was a shorter wait for an appointment by eVisit versus in-person (mean 59.98 [SD 48.36] days vs mean 78.36 [SD 50.54] days; P<.001). The eVisit was also shorter, taking on an average of only 10 min to deliver follow-up care with a high degree of patient satisfaction versus 90 (60-112) min for in-person care. The total time saved by patients per eVisit was 80 (50-102) min, 44 (21-69) min of which was travel time. Travel distance avoided by the patients was 30.1 km (11.2-82.2). The estimated total out-of-pocket cost savings for patients per eVisit was Can $52.83 (31.26-94.53). The estimated savings (opportunity cost for in-person outpatient care) for our eVisit pilot project was Can $23,832-$28,584. The patient satisfaction with eVisits was very good compared with their prior personal experience with in-person outpatient care.
Conclusions: The eVisit program was well received by patients, deemed to be safe by physicians, and avoided unnecessary patient travel and expense. It also has the potential to reduce health care costs. We plan to scale the project within the department and the institution.
Keywords: eHealth; eVisit; health services accessibility; mobile health; telemedicine.
©Ramana Appireddy, Sana Khan, Chad Leaver, Cally Martin, Albert Jin, Bryce A Durafourt, Stephen L Archer. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 07.10.2019.
Conflict of interest statement
Conflicts of Interest: RA received internal grant funding for the eVisit pilot project from the Department of Medicine, Queen’s University.
Figures
References
-
- Sibley LM, Glazier RH. Reasons for self-reported unmet healthcare needs in Canada: a population-based provincial comparison. Healthc Policy. 2009 Aug;5(1):87–101. http://europepmc.org/abstract/MED/20676253 - PMC - PubMed
-
- Ronksley PE, Sanmartin C, Campbell DJ, Weaver RG, Allan GM, McBrien KA, Tonelli M, Manns BJ, Hennessy D, Hemmelgarn BR. Perceived barriers to primary care among western Canadians with chronic conditions. Health Rep. 2014 Apr;25(4):3–10. http://www.statcan.gc.ca/pub/82-003-x/2014004/article/11923-eng.pdf 82-003-X201400411923 - PubMed
-
- Gibbard R. Canadian Medical Association. 2018. [2019-01-24]. Meeting the Care Needs of Canada’s Aging Population http://live-cma-ca.pantheonsite.io/sites/default/files/pdf/Activities/Co...
-
- Canadian Institute for Health Information. 2011. [2019-01-23]. Health Care in Canada, 2011 - A Focus on Seniors and Aging https://secure.cihi.ca/free_products/HCIC_2011_seniors_report_en.pdf .
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
