

Pattern Recognition to Identify Stroke in the Cognitive Profile: Secondary Analyses of a Prospective Cohort Study
- PMID: 31593944
- PMCID: PMC6873083
- DOI: 10.1159/000503002
Pattern Recognition to Identify Stroke in the Cognitive Profile: Secondary Analyses of a Prospective Cohort Study
Abstract
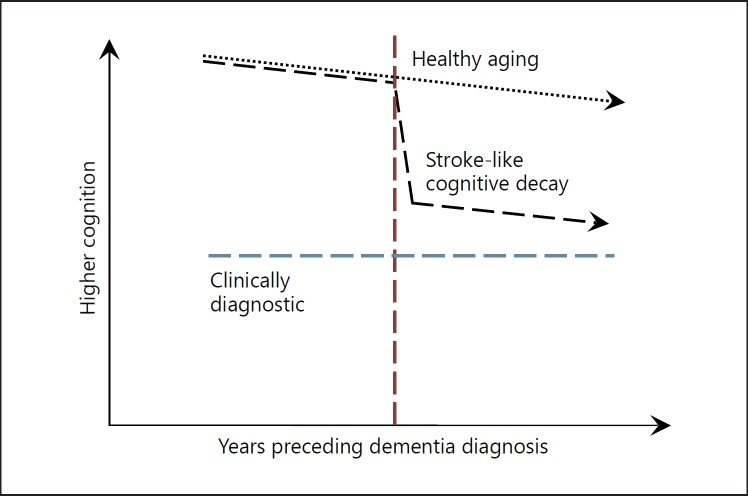
Background: Stroke can produce subtle changes in the brain that may produce symptoms that are too small to lead to a diagnosis. Noting that a lack of diagnosis may bias research estimates, the current study sought to examine the utility of pattern recognition relying on serial assessments of cognition to objectively identify stroke-like patterns of cognitive decline (pattern-detected stroke, p-stroke).
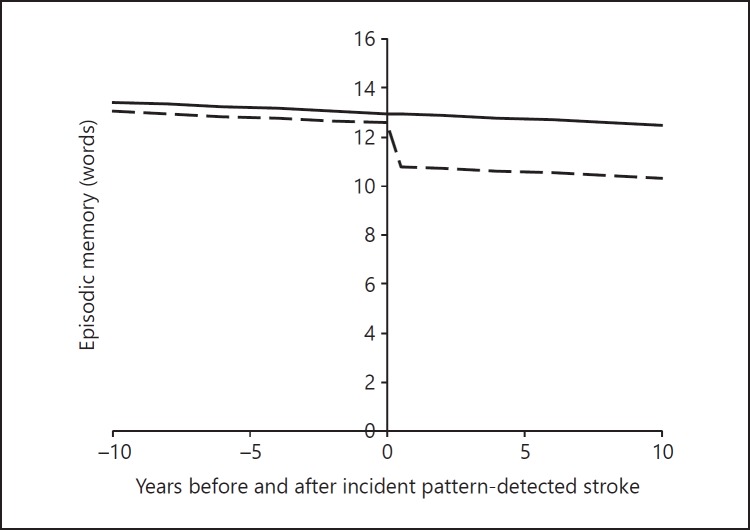
Methods: Secondary data analysis was conducted using participants with no reported history of stroke in the Health and Retirement Study, a large (n = 16,113) epidemiological study of cognitive aging among respondents aged 50 years and older that measured episodic memory consistently biennially between 1996 and 2014. Analyses were limited to participants with at least 4 serial measures of episodic memory. Occurrence and date of p-stroke events were identified utilizing pattern recognition to identify stepwise declines in cognition consistent with stroke. Descriptive statistics included the percentage of the population with p-stroke, the mean change in episodic memory resulting in stroke-positive testing, and the mean time between p-stroke and first major diagnosed stroke. Statistical analyses comparing cases of p-stroke with reported major stroke relied on the area under the receiver-operating curve (AUC). Longitudinal modeling was utilized to examine rates of change in those with/without major stroke after adjusting for demographics.
Results: The pattern recognition protocol identified 7,499 p-strokes that went unreported. On average, individuals with p-stroke declined in episodic memory by 1.986 (SD = 0.023) words at the inferred time of stroke. The resulting pattern recognition protocol was able to identify self--reported major stroke (AUC = 0.58, 95% CI = 0.57-0.59, p < 0.001). In those with a reported major stroke, p-stroke events were detectable on average 4.963 (4.650-5.275) years (p < 0.001) before diagnosis was first reported. The incidence of p-stroke was 40.23/1,000 (95% CI = 39.40-41.08) person-years. After adjusting for sex, age was associated with the incidence of p-stroke and major stroke at similar rates.
Conclusions: This is the first study to propose utilizing pattern recognition to identify the incidence and timing of p-stroke. Further work is warranted examining the clinical utility of pattern recognition in identifying p-stroke in longitudinal cognitive profiles.
Keywords: Adaptive diagnostics; Cerebrovascular diseases; Neuroepidemiology; Pattern recognition.
© 2019 The Author(s) Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest, financial or otherwise, to disclose.
Figures
References
-
- Gorelick PB, Scuteri A, Black SE, Decarli C, Greenberg SM, Iadecola C, et al. American Heart Association Stroke Council, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association. Stroke. 2011 Sep;42((9)):2672–713. - PMC - PubMed
-
- Howard VJ, McClure LA, Meschia JF, Pulley L, Orr SC, Friday GH. High prevalence of stroke symptoms among persons without a diagnosis of stroke or transient ischemic attack in a general population: the REasons for Geographic And Racial Differences in Stroke (REGARDS) study. Arch Intern Med. 2006 Oct;166((18)):1952–8. - PubMed
-
- Ince PG, Minett T, Forster G, Brayne C, Wharton SB, Function MR, et al. Medical Research Council Cognitive Function and Ageing Neuropathology Study Microinfarcts in an older population-representative brain donor cohort (MRC CFAS): Prevalence, relation to dementia and mobility, and implications for the evaluation of cerebral Small Vessel Disease. Neuropathol Appl Neurobiol. 2017 Aug;43((5)):409–18. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
