

Advances in Optical Coherence Tomography and Confocal Laser Endomicroscopy in Pulmonary Diseases
- PMID: 31593955
- PMCID: PMC7212699
- DOI: 10.1159/000503261
Advances in Optical Coherence Tomography and Confocal Laser Endomicroscopy in Pulmonary Diseases
Abstract
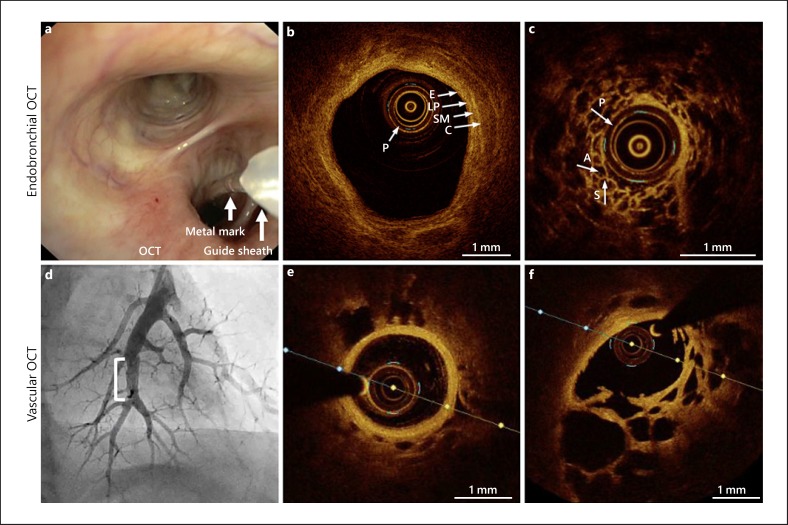
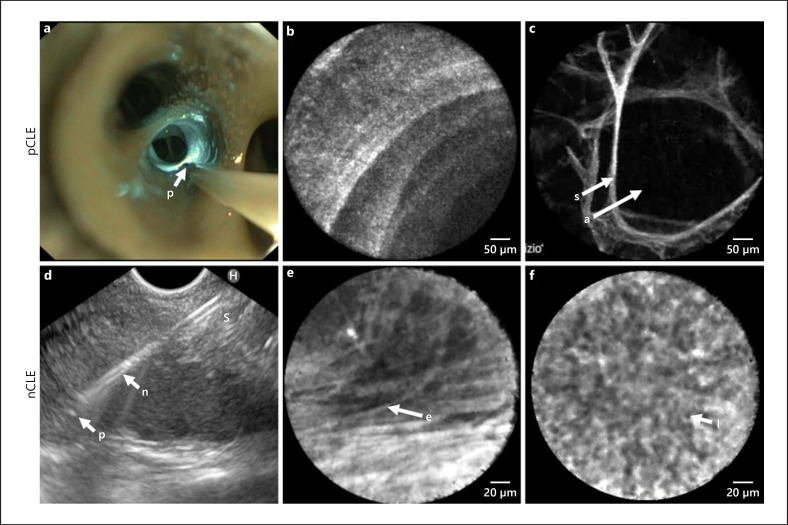
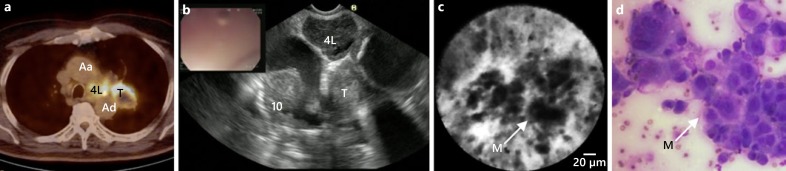
Diagnosing and monitoring pulmonary diseases is highly dependent on imaging, physiological function tests and tissue sampling. Optical coherence tomography (OCT) and confocal laser endomicroscopy (CLE) are novel imaging techniques with near-microscopic resolution that can be easily and safely combined with conventional bronchoscopy. Disease-related pulmonary anatomical compartments can be visualized, real time, using these techniques. In obstructive lung diseases, airway wall layers and related structural remodelling can be identified and quantified. In malignant lung disease, normal and malignant areas of the central airways, lung parenchyma, lymph nodes and pleura can be discriminated. A growing number of interstitial lung diseases (ILDs) have been visualized using OCT or CLE. Several ILD-associated structural changes can be imaged: fibrosis, cellular infiltration, bronchi(ol)ectasis, cysts and microscopic honeycombing. Although not yet implemented in clinical practice, OCT and CLE have the potential to improve detection and monitoring pulmonary diseases and can contribute in unravelling the pathophysiology of disease and mechanism of action of novel treatments. Indeed, assessment of the airway wall layers with OCT might be helpful when evaluating treatments targeting airway remodelling. By visualizing individual malignant cells, CLE has the potential as a real-time lung cancer detection tool. In the future, both techniques could be combined with laser-enhanced fluorescent-labelled tracer detection. This review discusses the value of OCT and CLE in pulmonary medicine by summarizing the current evidence and elaborating on future perspectives.
Keywords: Bronchoscopy; Confocal laser endomicroscopy; Interstitial lung disease; Lung cancer; Obstructive lung disease; Optical coherence tomography.
The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The department of pulmonology received material support from St Jude Medical Inc., St. Paul, MN, USA/Abbott, Illinois and an unrestricted research grant from Mauna Kea Technologies, Paris, France.
Figures




References
-
- Wijmans L, d'Hooghe JN, Bonta PI, Annema JT. Optical coherence tomography and confocal laser endomicroscopy in pulmonary diseases. Curr Opin Pulm Med. 2017 May;23((3)):275–83. - PubMed
-
- Tearney GJ, Brezinski ME, Bouma BE, Boppart SA, Pitris C, Southern JF, et al. In vivo endoscopic optical biopsy with optical coherence tomography. Science. 1997 Jun;276((5321)):2037–9. - PubMed
-
- Fercher AF, Hitzenberger CK, Drexler W, Kamp G, Sattmann H. In vivo optical coherence tomography. Am J Ophthalmol. 1993 Jul;116((1)):113–4. - PubMed
-
- Swanson EA, Izatt JA, Hee MR, Huang D, Lin CP, Schuman JS, et al. In vivo retinal imaging by optical coherence tomography. Opt Lett. 1993 Nov;18((21)):1864–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
