

Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults
- PMID: 31594780
- PMCID: PMC6780322
- DOI: 10.1136/bmj.l5367
Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults
Abstract
Objective: To estimate the risk of acute myocardial infarction (AMI) or stroke in adults with non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH).
Design: Matched cohort study.
Setting: Population based, electronic primary healthcare databases before 31 December 2015 from four European countries: Italy (n=1 542 672), Netherlands (n=2 225 925), Spain (n=5 488 397), and UK (n=12 695 046).
Participants: 120 795 adults with a recorded diagnosis of NAFLD or NASH and no other liver diseases, matched at time of NAFLD diagnosis (index date) by age, sex, practice site, and visit, recorded at six months before or after the date of diagnosis, with up to 100 patients without NAFLD or NASH in the same database.
Main outcome measures: Primary outcome was incident fatal or non-fatal AMI and ischaemic or unspecified stroke. Hazard ratios were estimated using Cox models and pooled across databases by random effect meta-analyses.
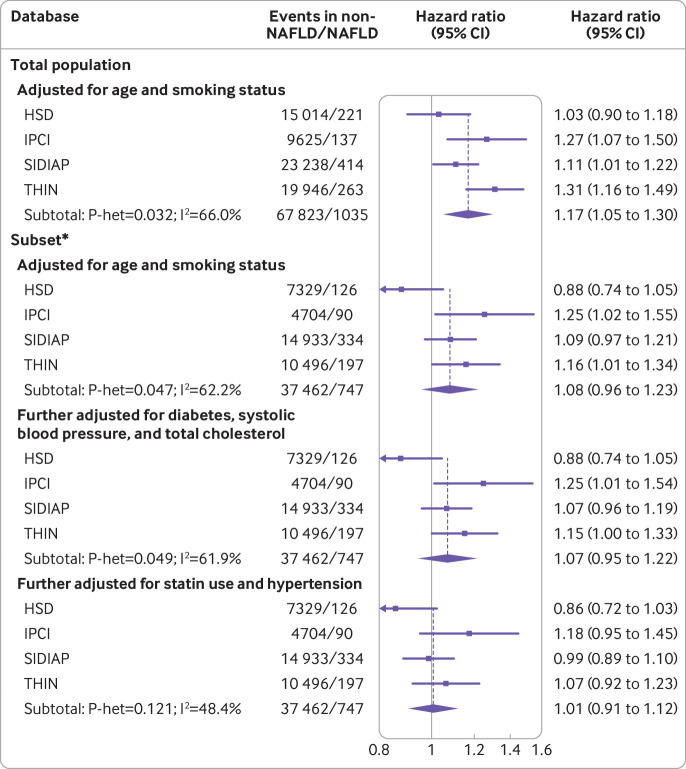
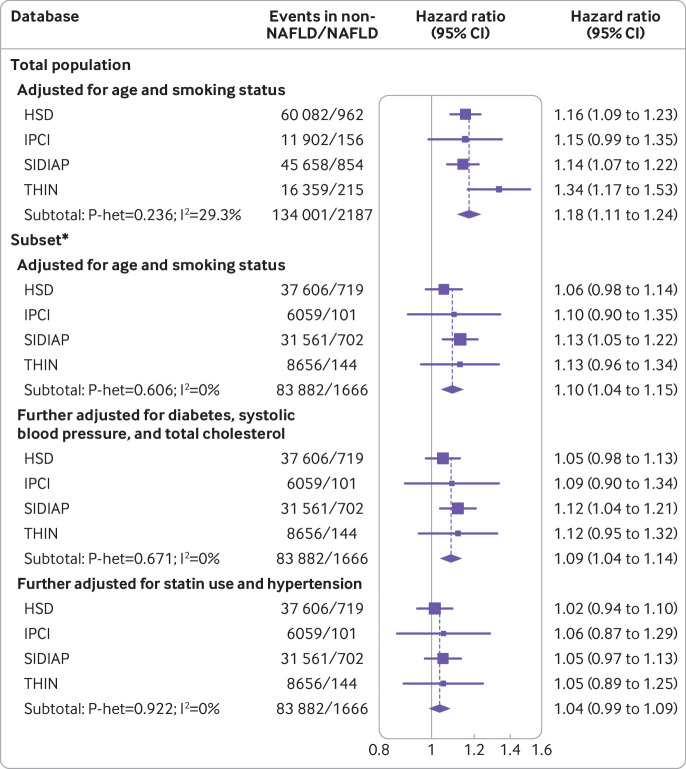
Results: 120 795 patients with recorded NAFLD or NASH diagnoses were identified with mean follow-up 2.1-5.5 years. After adjustment for age and smoking the pooled hazard ratio for AMI was 1.17 (95% confidence interval 1.05 to 1.30; 1035 events in participants with NAFLD or NASH, 67 823 in matched controls). In a group with more complete data on risk factors (86 098 NAFLD and 4 664 988 matched controls), the hazard ratio for AMI after adjustment for systolic blood pressure, type 2 diabetes, total cholesterol level, statin use, and hypertension was 1.01 (0.91 to 1.12; 747 events in participants with NAFLD or NASH, 37 462 in matched controls). After adjustment for age and smoking status the pooled hazard ratio for stroke was 1.18 (1.11 to 1.24; 2187 events in participants with NAFLD or NASH, 134 001 in matched controls). In the group with more complete data on risk factors, the hazard ratio for stroke was 1.04 (0.99 to 1.09; 1666 events in participants with NAFLD, 83 882 in matched controls) after further adjustment for type 2 diabetes, systolic blood pressure, total cholesterol level, statin use, and hypertension.
Conclusions: The diagnosis of NAFLD in current routine care of 17.7 million patient appears not to be associated with AMI or stroke risk after adjustment for established cardiovascular risk factors. Cardiovascular risk assessment in adults with a diagnosis of NAFLD is important but should be done in the same way as for the general population.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: MA reports being contracted by SRG to work for GlaxoSmithKline and received a salary from GSK, including bonus. JF-B and DW are paid employees at GlaxoSmithKline and receive salaries, including bonuses. AKL is a paid employee at Pfizer and receives a salary, including bonus. DP-A reports unrestricted research grants from UCB, Amgen, and Servier, and consultancy fees from UCB Pharma paid to his department. DA reports as a paid employee of IQVIA has provided consultancy and advice to many pharmaceutical companies on undertaking outcomes studies using real world evidence. PE and SK report they are paid employees and stock holders of GlaxoSmithKline. NS reports personal fees from AstraZeneca, Amgen, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Janssen, and Sanofi and a grant from Boehringer Ingelheim. WA reports consultancy and sponsored lectures from Gilead, GlaxoSmithKline, Intercept IQVIA, and UCB Pharma.
Figures
Comment in
-
Studies on non-alcoholic fatty liver disease should stratify by disease severity.BMJ. 2019 Nov 22;367:l6495. doi: 10.1136/bmj.l6495. BMJ. 2019. PMID: 31757812 No abstract available.
-
Is Nonalcoholic Fatty Liver Disease Not a Risk Factor for Cardiovascular Disease: Not Yet Time for a Change of Heart.Hepatology. 2020 May;71(5):1867-1869. doi: 10.1002/hep.31156. Hepatology. 2020. PMID: 32012311 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical