

Plasma Desmosine and Abdominal Aortic Aneurysm Disease
- PMID: 31595818
- PMCID: PMC6818029
- DOI: 10.1161/JAHA.119.013743
Plasma Desmosine and Abdominal Aortic Aneurysm Disease
Abstract
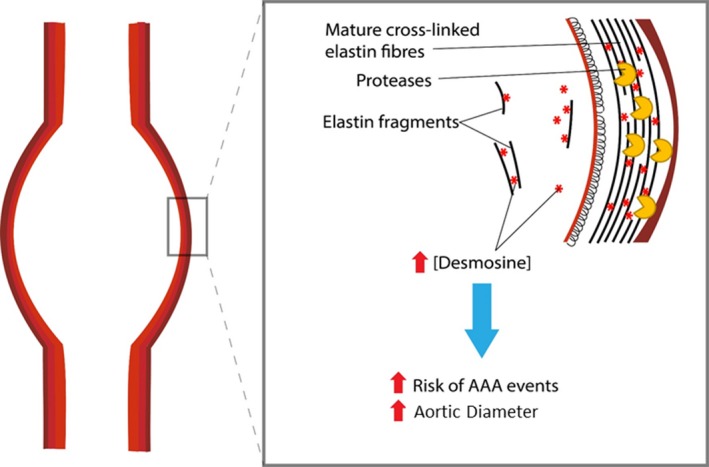
Background It is recognized that factors beyond aortic size are important in predicting outcome in abdominal aortic aneurysm (AAA) disease. AAA is characterized by the breakdown of elastin within the aortic tunica media, leading to aortic dilatation and rupture. The aim of this study was to investigate the association of plasma desmosine (pDES), an elastin-specific degradation product, with disease severity and clinical outcome in patients with AAA. Methods and Results We measured pDES and serum biomarker concentrations in 507 patients with AAAs (94% men; mean age, 72.4±6.1 years; mean AAA diameter, 48±8 mm) and 162 control subjects (100% men; mean age, 71.5±4.4 years) from 2 observational cohort studies. In the longitudinal cohort study (n=239), we explored the incremental prognostic value of pDES on AAA events. pDES was higher in patients with AAA compared with control subjects (mean±SD: 0.46±0.22 versus 0.33±0.16 ng/mL; P<0.001) and had the strongest correlation with AAA diameter (r=0.39; P<0.0001) of any serum biomarker. After adjustment for baseline AAA diameter, pDES was associated with an AAA event (hazard ratio, 2.03 per SD increase [95% CI, 1.02-4.02]; P=0.044). In addition to AAA diameter, pDES provided incremental improvement in risk stratification (continuous net reclassification improvement, 34.4% [95% CI, -10.8% to 57.5%; P=0.09]; integrated discrimination improvement, 0.04 [95% CI, 0.00-0.15; P=0.050]). Conclusions pDES concentrations predict disease severity and clinical outcomes in patients with AAA. Clinical Trial Registration http://www.isrctn.com. Unique identifier: ISRCTN76413758.
Keywords: abdominal aortic aneurysm; aortic rupture; desmosine; elastin.
Figures




References
-
- Benson RA, Poole R, Murray S, Moxey P, Loftus IM. Screening results from a large United Kingdom abdominal aortic aneurysm screening center in the context of optimizing United Kingdom National Abdominal Aortic Aneurysm Screening Programme protocols. J Vasc Surg. 2016;63:301–304. - PubMed
-
- Abdulameer H, Al Taii H, Al‐Kindi SG, Milner R. Epidemiology of fatal ruptured aortic aneurysms in the United States (1999–2016). J Vasc Surg. 2019;69:378–384.e2. - PubMed
-
- Cosford PA, Leng GC. Screening for abdominal aortic aneurysm. Cochrane Database Syst Rev. 2007:CD002945. - PubMed
-
- Lederle FA. The last (randomized) word on screening for abdominal aortic aneurysms. JAMA Intern Med. 2016;176:1767–1768. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
