

Incidence of Initial Renal Replacement Therapy Over the Course of Kidney Disease in Children
- PMID: 31595948
- PMCID: PMC7036655
- DOI: 10.1093/aje/kwz220
Incidence of Initial Renal Replacement Therapy Over the Course of Kidney Disease in Children
Abstract
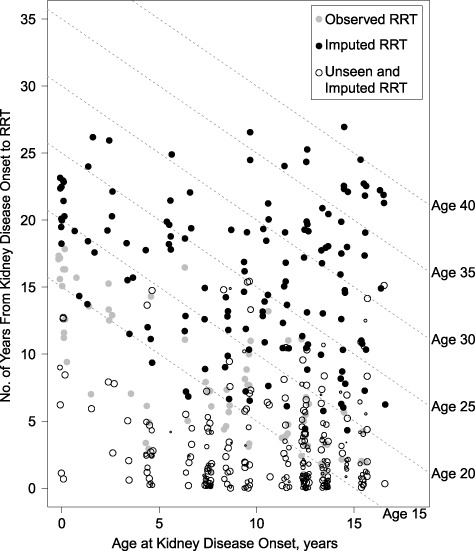
The Chronic Kidney Disease in Children Study, a prospective cohort study with data collected from 2003 to 2018, provided the first opportunity to characterize the incidence of renal replacement therapy (RRT) initiation over the life course of pediatric kidney diseases. In the current analysis, parametric generalized gamma models were fitted and extrapolated for RRT overall and by specific treatment modality (dialysis or preemptive kidney transplant). Children were stratified by type of diagnosis: nonglomerular (mostly congenital; n = 650), glomerular-hemolytic uremic syndrome (HUS; n = 49), or glomerular-non-HUS (heterogeneous childhood onset; n = 216). Estimated durations of time to RRT after disease onset for 99% of the nonglomerular and glomerular-non-HUS groups were 42.5 years (95% confidence interval (CI): 31.0, 54.1) and 25.4 years (95% CI: 14.9, 36.0), respectively. Since onset for the great majority of children in the nonglomerular group was congenital, disease duration equated with age. A simulation-based estimate of age at RRT for 99% of the glomerular population was 37.9 years (95% CI: 33.6, 63.2). These models performed well in cross-validation. Children with glomerular disease received dialysis earlier and were less likely to have a preemptive kidney transplant, while the timing and proportions of dialysis and transplantation were similar for the nonglomerular group. These diagnosis-specific estimates provide insight into patient-centered prognostic information and can assist in RRT planning efforts for children with moderate-to-severe kidney disease who are receiving regular specialty care.
Keywords: dialysis; kidney disease; kidney transplantation; pediatrics; prospective studies; renal insufficiency; renal replacement therapy.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health.
Figures

References
-
- Eckardt K-U, Coresh J, Devuyst O, et al. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382(9887):158–169. - PubMed
