

Longitudinal Associations Between Income Changes and Incident Cardiovascular Disease: The Atherosclerosis Risk in Communities Study
- PMID: 31596441
- PMCID: PMC6802267
- DOI: 10.1001/jamacardio.2019.3788
Longitudinal Associations Between Income Changes and Incident Cardiovascular Disease: The Atherosclerosis Risk in Communities Study
Abstract
Importance: Higher income is associated with lower incident cardiovascular disease (CVD). However, there is limited research on the association between changes in income and incident CVD.
Objective: To examine the association between change in household income and subsequent risk of CVD.
Design, setting, and participants: The Atherosclerosis Risk In Communities (ARIC) study is an ongoing, prospective cohort of 15 792 community-dwelling men and women, of mostly black or white race, from 4 centers in the United States (Jackson, Mississippi; Washington County, Maryland; suburbs of Minneapolis, Minnesota; and Forsyth County, North Carolina), beginning in 1987. For our analysis, participants were followed up until December 31, 2016.
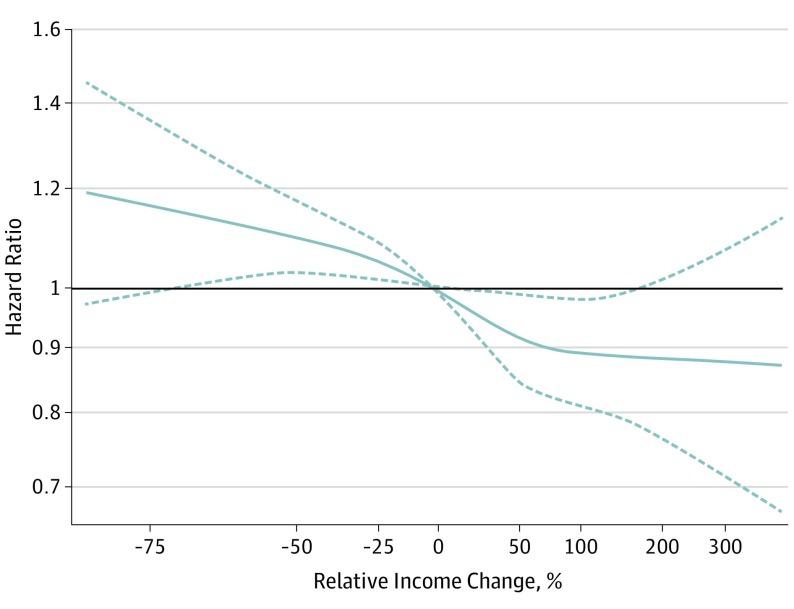
Exposures: Participants were categorized based on whether their household income dropped by more than 50% (income drop), remained unchanged/changed less than 50% (income unchanged), or increased by more than 50% (income rise) over a mean (SD) period of approximately 6 (0.3) years between ARIC visit 1 (1987-1989) and visit 3 (1993-1995).
Main outcomes and measures: Our primary outcome was incidence of CVD after ARIC visit 3, including myocardial infarction (MI), fatal coronary heart disease, heart failure (HF), or stroke during a mean (SD) of 17 (7) years. Analyses were adjusted for sociodemographic variables, health behaviors, and CVD biomarkers.
Results: Of the 8989 included participants (mean [SD] age at enrollment was 53 [6] years, 1820 participants were black [20%], and 3835 participants were men [43%]), 900 participants (10%) experienced an income drop, 6284 participants (70%) had incomes that remained relatively unchanged, and 1805 participants (20%) experienced an income rise. After full adjustment, those with an income drop experienced significantly higher risk of incident CVD compared with those whose incomes remained relatively unchanged (hazard ratio, 1.17; 95% CI, 1.03-1.32). Those with an income rise experienced significantly lower risk of incident CVD compared with those whose incomes remained relatively unchanged (hazard ratio, 0.86; 95% CI, 0.77-0.96).
Conclusions and relevance: Income drop over 6 years was associated with higher risk of subsequent incident CVD over 17 years, while income rise over 6 years was associated with lower risk of subsequent incident CVD over 17 years. Health professionals should have greater awareness of the influence of income change on the health of their patients.
Conflict of interest statement
Figures


Comment in
-
The Influence of Social and Economic Factors on Heart Disease.JAMA Cardiol. 2019 Dec 1;4(12):1212-1213. doi: 10.1001/jamacardio.2019.3802. JAMA Cardiol. 2019. PMID: 31596424 No abstract available.
References
-
- Berkman LF, Kawachi I, Glymour MM. Social Epidemiology Second Edition. New York, NY: Oxford University Press; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
