

Risk of Pulmonary Embolism More Than 6 Weeks After Surgery Among Cancer-Free Middle-aged Patients
- PMID: 31596449
- PMCID: PMC6802263
- DOI: 10.1001/jamasurg.2019.3742
Risk of Pulmonary Embolism More Than 6 Weeks After Surgery Among Cancer-Free Middle-aged Patients
Abstract
Importance: The risk of postoperative pulmonary embolism has been reported to be highest during the first 5 weeks after surgery. However, how long the excess risk of postoperative pulmonary embolism persists remains unknown.
Objective: To assess the duration and magnitude of the late postoperative risk of pulmonary embolism among cancer-free middle-aged patients by the type of surgery.
Design, setting, and participants: Case-crossover analysis to compute the respective risks of pulmonary embolism after 6 types of surgery using data from a French national inpatient database, which covers a total of 203 million inpatient stays over an 8-year period between 2007 and 2014. Participants were cancer-free middle-aged adult patients (aged 45 to 64) with a diagnosis of a first pulmonary embolism.
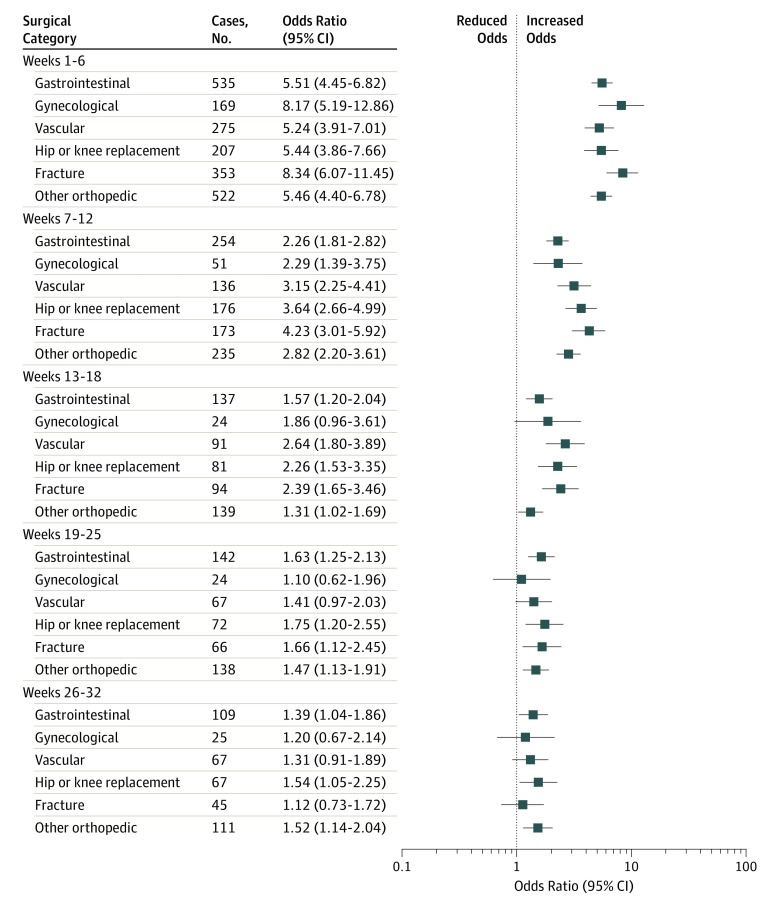
Exposures: Hospital admission for surgery. Surgical procedures were classified into 6 types: (1) vascular surgery, (2) gynecological surgery, (3) gastrointestinal surgery, (4) hip or knee replacement, (5) fractures, and (6) other orthopedic operations.
Main outcomes and measures: Diagnosis of a first pulmonary embolism.
Results: A total of 60 703 patients were included (35 766 [58.9%] male; mean [SD] age, 56.6 [6.0] years). The risk of postoperative pulmonary embolism was elevated for at least 12 weeks after all types of surgery and was highest during the immediate postoperative period (1 to 6 weeks). The excess risk of postoperative pulmonary embolism ranged from odds ratio (OR), 5.24 (95% CI, 3.91-7.01) for vascular surgery to OR, 8.34 (95% CI, 6.07-11.45) for surgery for fractures. The risk remained elevated from 7 to 12 weeks, with the OR ranging from 2.26 (95% CI, 1.81-2.82) for gastrointestinal operations to 4.23 (95% CI, 3.01-5.92) for surgery for fractures. The risk was not clinically significant beyond 18 weeks postsurgery for all types of procedures.
Conclusions and relevance: The risk of postoperative pulmonary embolism is elevated beyond 6 weeks postsurgery regardless of the type of procedure. The persistence of this excess risk suggests that further randomized clinical trials are required to evaluate whether the duration of postoperative prophylactic anticoagulation should be extended and to define the optimal duration of treatment with regard to both the thrombotic and bleeding risks.
Conflict of interest statement
Figures


Comment in
-
Are We Really Supposed to Start Giving Venous Thromboembolism Prophylaxis for a Month After Outpatient Surgery?JAMA Surg. 2019 Dec 1;154(12):1133. doi: 10.1001/jamasurg.2019.3753. JAMA Surg. 2019. PMID: 31596432 No abstract available.
