

Association of Estimated Pulse Wave Velocity With Survival: A Secondary Analysis of SPRINT
- PMID: 31596491
- PMCID: PMC6802234
- DOI: 10.1001/jamanetworkopen.2019.12831
Association of Estimated Pulse Wave Velocity With Survival: A Secondary Analysis of SPRINT
Abstract
Importance: Aortic stiffness, as assessed by carotid-femoral pulse wave velocity, is an independent predictor of future events in individuals with hypertension. Recent data suggest a predictive role of estimated pulse wave velocity (ePWV) calculated by previously published equations using age and blood pressure in future events in individuals with hypertension.
Objective: To investigate whether ePWV and its response to treatment predict survival in the Systolic Blood Pressure Intervention Trial (SPRINT).
Design, setting, and participants: This exploratory, hypothesis-generating, post hoc secondary analysis conducted from October 1, 2018, to August 31, 2019, examined data from 9361 participants in SPRINT and calculated ePWV at baseline and at 12 months. Adjusted hazard ratios (HRs) with 95% CIs of ePWV per 1 SD were estimated using Cox proportional hazards regression models. A total of 8450 patients were assigned to 4 groups according to their treatment allocation and their response in ePWV after 12 months.
Interventions: Participants were assigned a systolic blood pressure target of less than 120 mm Hg (intensive treatment) or less than 140 mm Hg (standard treatment).
Main outcomes and measures: The primary composite cardiovascular outcome was myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes.
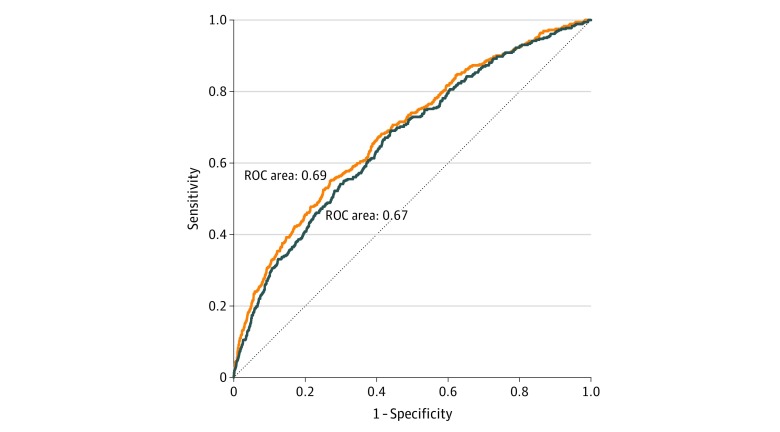
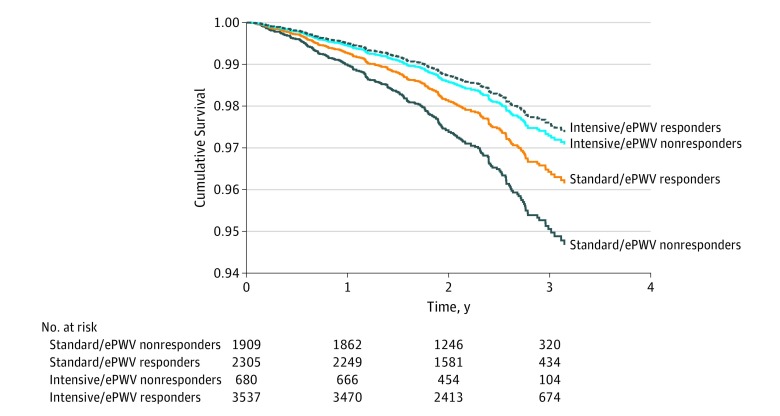
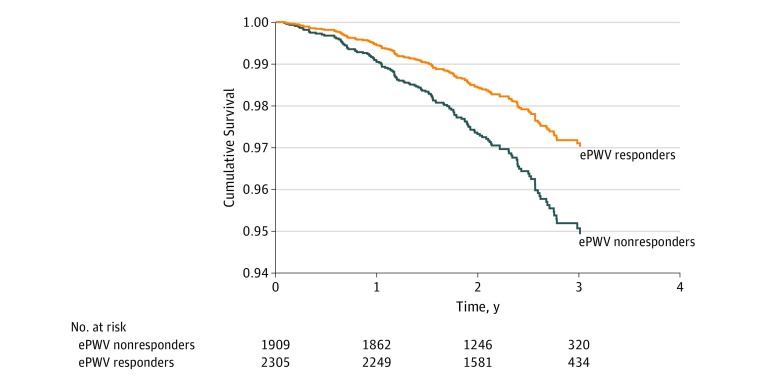
Results: In the SPRINT population (3332 women and 6029 men; mean [SD] age, 67.9 [9.4] years), ePWV predicted the primary outcome (HR, 1.30 [95% CI, 1.17-1.43]; P < .001) and all-cause death (HR, 1.65 [95% CI, 1.46-1.86]; P < .001) independent of the Framingham Risk Score. Estimated pulse wave velocity improved the C statistic model for the primary outcome from 0.676 (95% CI, 0.65-0.70) to 0.683 (95% CI, 0.66-0.71; P = .049) and improved the C statistic model for all-cause death from 0.67 (95% CI, 0.64-0.69) to 0.69 (95% CI, 0.66-0.72; P = .03). Net reclassification index indicated improvement in risk discrimination for survival compared with the Framingham Risk Score (categorical net reclassification index = 0.111; P < .001). Regarding response to treatment, intensive treatment was superior to standard treatment only when it was accompanied with a response in ePWV at the first year, while, within the standard treatment group, individuals whose ePWV responded to antihypertensive treatment had improved all-cause mortality, with a 42% lower risk of death compared with nonresponders (HR, 0.58 [95% CI, 0.36-0.94]; P = .03); effects were independent of changes in systolic blood pressure.
Conclusions and relevance: These results suggest that, in the SPRINT trial, ePWV predicted outcomes independent of the Framingham Risk Score, indicating an incremental role of markers of aortic stiffness on cardiovascular risk. Better survival of individuals whose ePWV responded to antihypertensive treatment independently of systolic blood pressure reduction suggests a role of markers of aortic stiffness as effective treatment targets in individuals with hypertension.
Conflict of interest statement
Figures
References
-
- Terentes-Printzios D, Vlachopoulos C, Xaplanteris P, et al. Cardiovascular risk factors accelerate progression of vascular aging in the general population: results from the CRAVE study (Cardiovascular Risk Factors Affecting Vascular Age). Hypertension. 2017;70(5):1057-1064. doi: 10.1161/HYPERTENSIONAHA.117.09633 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
