

ILC3 deficiency and generalized ILC abnormalities in DOCK8-deficient patients
- PMID: 31596517
- PMCID: PMC7141948
- DOI: 10.1111/all.14081
ILC3 deficiency and generalized ILC abnormalities in DOCK8-deficient patients
Abstract
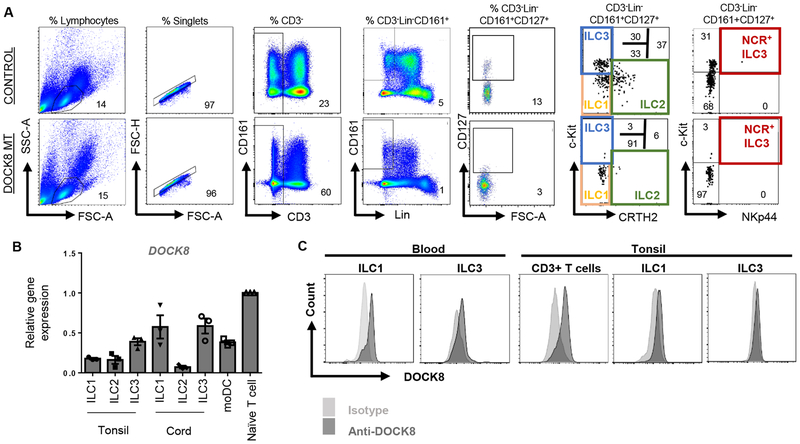
Background: Dedicator of cytokinesis 8 (DOCK8) deficiency is the main cause of the autosomal recessive hyper-IgE syndrome (HIES). We previously reported the selective loss of group 3 innate lymphoid cell (ILC) number and function in a Dock8-deficient mouse model. In this study, we sought to test whether DOCK8 is required for the function and maintenance of ILC subsets in humans.
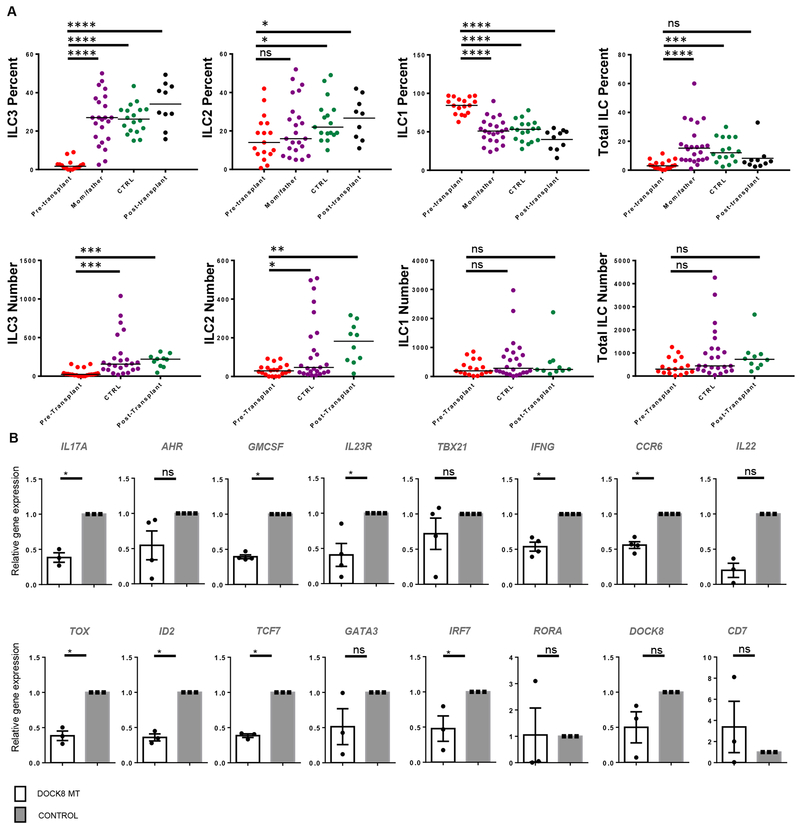
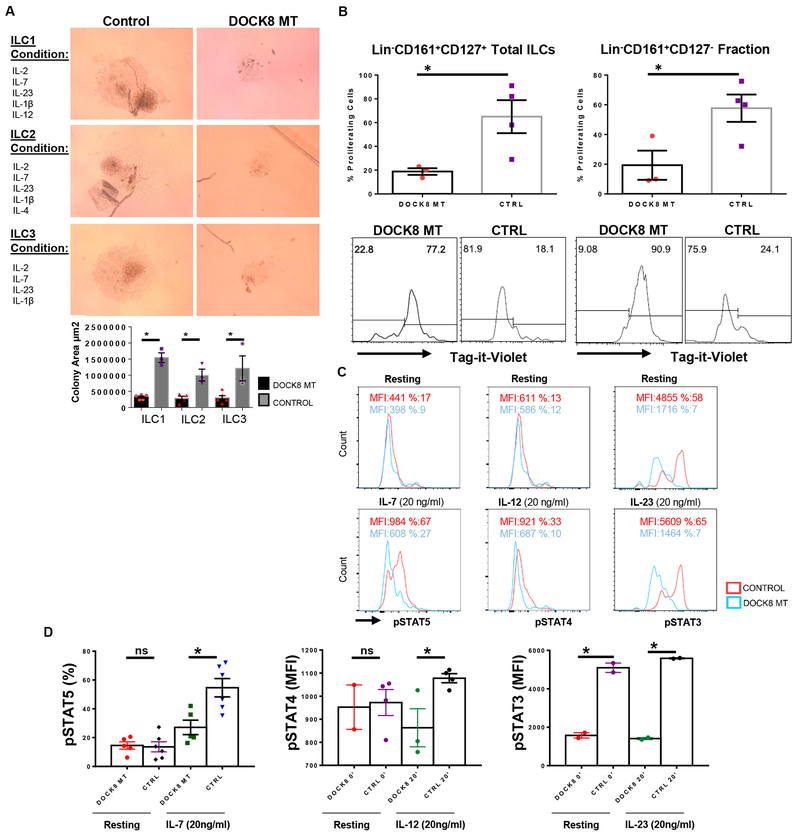
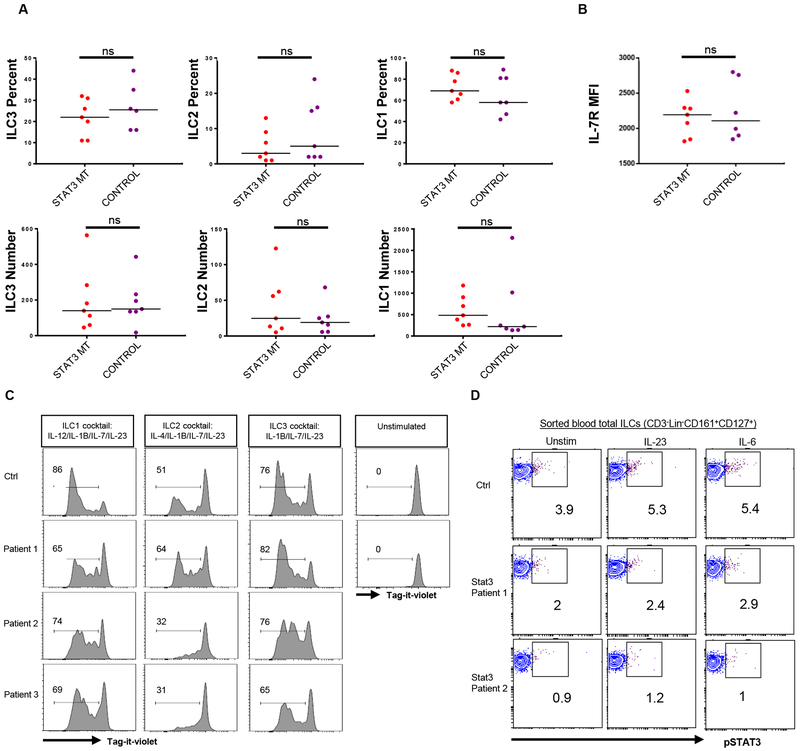
Methods: Peripheral blood ILC1-3 subsets of 16 DOCK8-deficient patients recruited at the pretransplant stage, and seven patients with autosomal dominant (AD) HIES due to STAT3 mutations, were compared with those of healthy controls or post-transplant DOCK8-deficient patients (n = 12) by flow cytometry and real-time qPCR. Sorted total ILCs from DOCK8- or STAT3-mutant patients and healthy controls were assayed for survival, apoptosis, proliferation, and activation by IL-7, IL-23, and IL-12 by cell culture, flow cytometry, and phospho-flow assays.
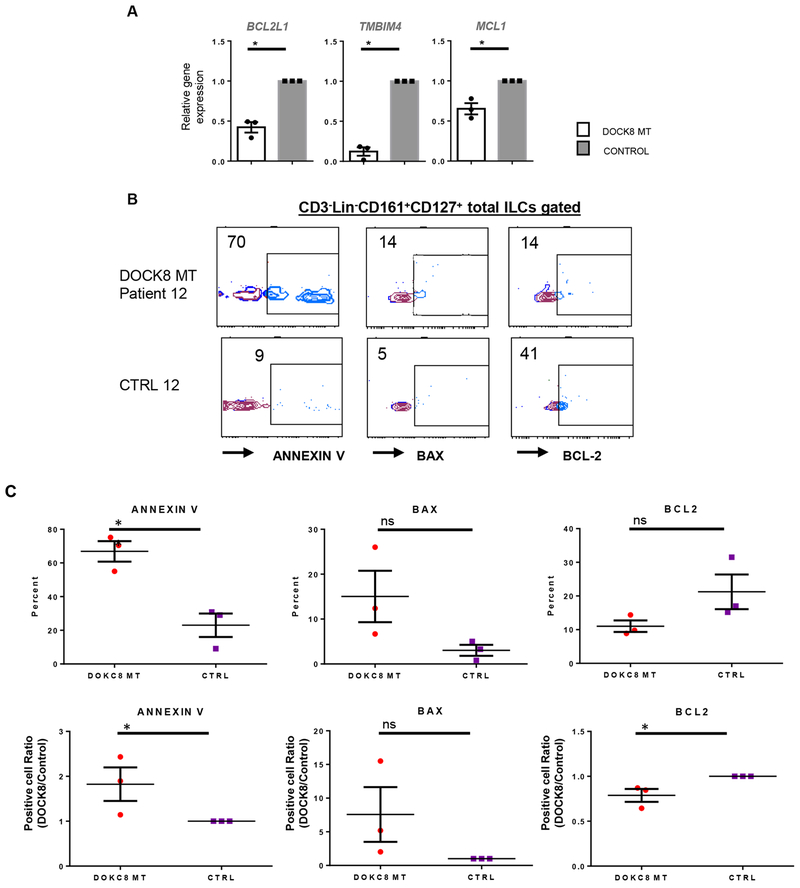
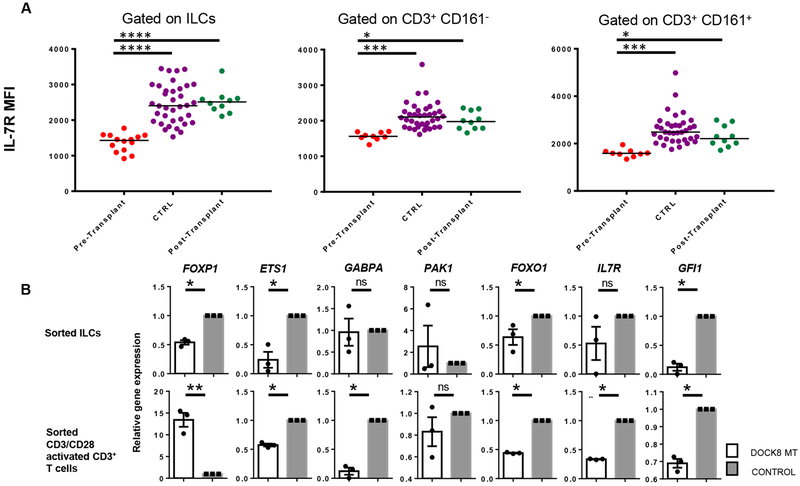
Results: DOCK8-deficient but not STAT3-mutant patients exhibited a profound depletion of ILC3s, and to a lesser extent ILC2s, in their peripheral blood. DOCK8-deficient ILC1-3 subsets had defective proliferation, expressed lower levels of IL-7R, responded less to IL-7, IL-12, or IL-23 cytokines, and were more prone to apoptosis compared with those of healthy controls.
Conclusion: DOCK8 regulates human ILC3 expansion and survival, and more globally ILC cytokine signaling and proliferation. DOCK8 deficiency leads to loss of ILC3 from peripheral blood. ILC3 deficiency may contribute to the susceptibility of DOCK8-deficient patients to infections.
Keywords: DOCK8; Hyper-IgE syndrome (HIES); ILC; ILC3; STAT3.
© 2019 EAACI and John Wiley and Sons A/S. Published by John Wiley and Sons Ltd.
Conflict of interest statement
Figures
References
-
- Aydin SE, Kilic SS, Aytekin C, Kumar A, Porras O, Kainulainen L et al. DOCK8 Deficiency: Clinical and Immunological Phenotype and Treatment Options - a Review of 136 Patients. J Clin Immunol 2015;35:189–198. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
