

Psychiatric morbidity and suicidal behaviour in low- and middle-income countries: A systematic review and meta-analysis
- PMID: 31597983
- PMCID: PMC6785653
- DOI: 10.1371/journal.pmed.1002905
Psychiatric morbidity and suicidal behaviour in low- and middle-income countries: A systematic review and meta-analysis
Abstract
Background: Psychiatric disorders are reported to be present in 80% to 90% of suicide deaths in high-income countries (HIC), but this association is less clear in low- and middle-income countries (LMIC). There has been no previous systematic review of this issue in LMIC. The current study aims to estimate the prevalence of psychiatric morbidity in individuals with suicidal behaviour in LMIC.
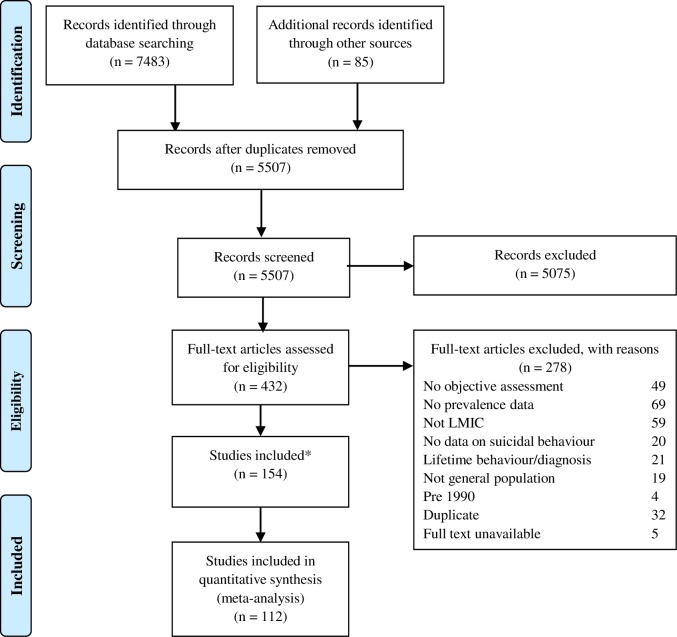
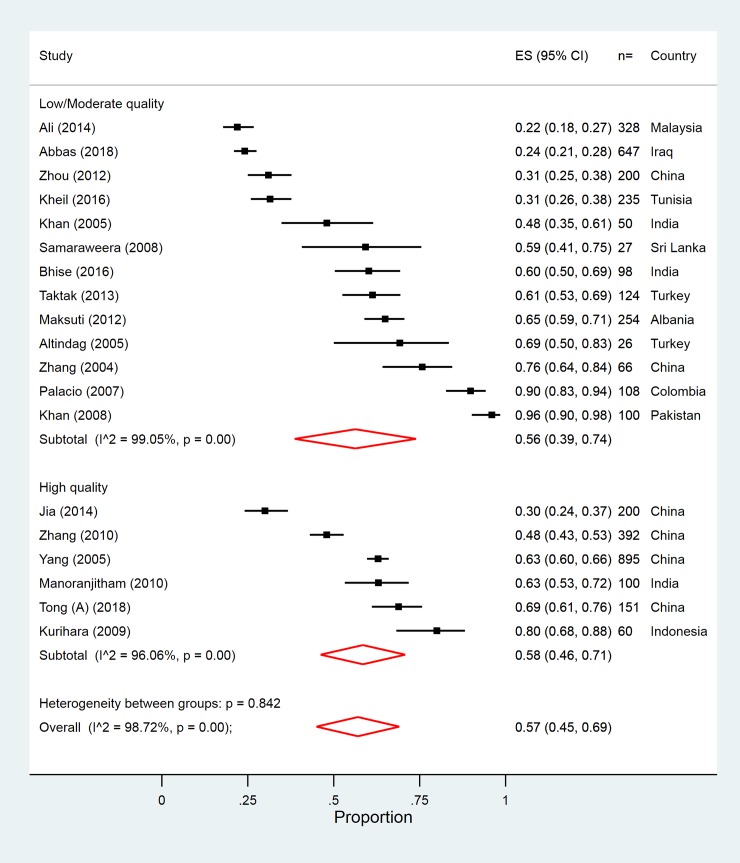
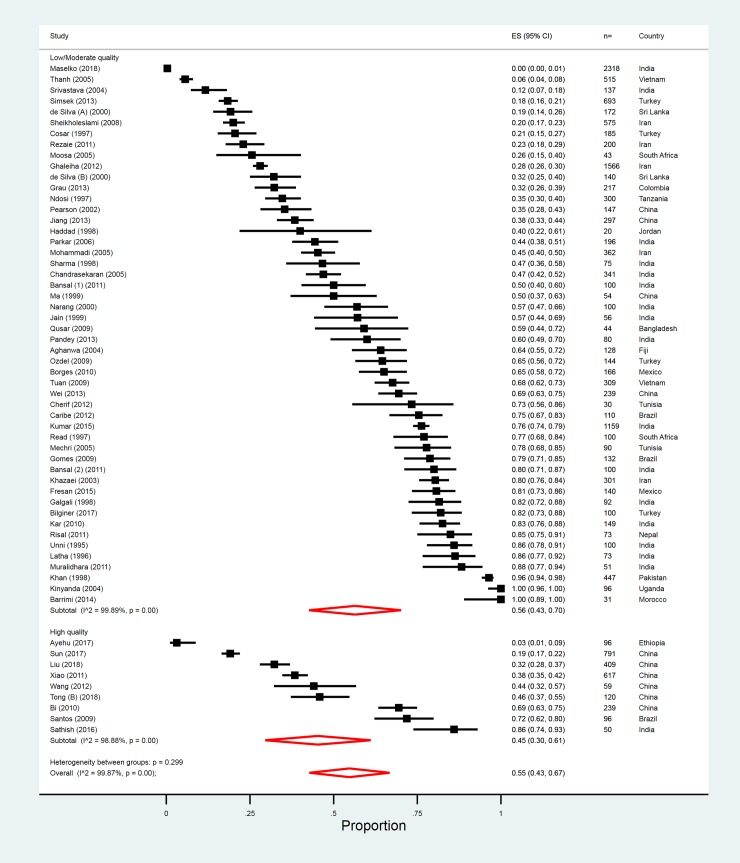
Methods and findings: PubMed, PsycINFO, and EMBASE searches were conducted to identify quantitative research papers (any language) between 1990 and 2018 from LMIC that reported on the prevalence of psychiatric morbidity in suicidal behaviour. We used meta-analytic techniques to generate pooled estimates for any psychiatric disorder and specific diagnosis based on International classification of disease (ICD-10) criteria. A total of 112 studies (154 papers) from 26 LMIC (India: 25%, China: 15%, and other LMIC: 60%) were identified, including 18 non-English articles. They included 30,030 individuals with nonfatal suicidal behaviour and 4,996 individuals who had died by suicide. Of the 15 studies (5 LMIC) that scored highly on our quality assessment, prevalence estimates for psychiatric disorders ranged between 30% and 80% in suicide deaths and between 3% and 86% in those who engaged in nonfatal suicidal behaviour. There was substantial heterogeneity between study estimates. Fifty-eight percent (95% CI 46%-71%) of those who died by suicide and 45% (95% CI 30%-61%) of those who engaged in nonfatal suicidal behaviour had a psychiatric disorder. The most prevalent disorder in both fatal and nonfatal suicidal behaviour was mood disorder (25% and 21%, respectively). Schizophrenia and related disorders were identified in 8% (4%-12%) of those who died by suicide and 7% (3%-11%) of those who engaged in nonfatal suicidal behaviour. In nonfatal suicidal behaviour, anxiety disorders, and substance misuse were identified in 19% (1%-36%) and 11% (7%-16%) of individuals, respectively. This systematic review was limited by the low number of high-quality studies and restricting our searches to databases that mainly indexed English language journals.
Conclusions: Our findings suggest a possible lower prevalence of psychiatric disorders in suicidal behaviour in LMIC. We found very few high-quality studies and high levels of heterogeneity in pooled estimates of psychiatric disorder, which could reflect differing study methods or real differences. There is a clear need for more robust evidence in order for LMIC to strike the right balance between community-based and mental health focussed interventions.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: NK chairs and contributes to a number of guidelines for self-harm and suicidal behaviour and sits on the main government advisory group for suicide prevention in England. NK and DK also advised the Sri Lankan Ministry of Health on their suicide prevention strategy. NK receives research funding from government and charity sources. NK does not receive industry funding or personal remuneration.
Figures
References
-
- World Health Organisation. Preventing suicide—A global imperative Geneva: WHO, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
