

Changes in cortical motor outputs after a motor relapse of multiple sclerosis
- PMID: 31598329
- PMCID: PMC6764060
- DOI: 10.1177/2055217319866480
Changes in cortical motor outputs after a motor relapse of multiple sclerosis
Abstract
Background: Motor recovery following a multiple sclerosis (MS) relapse depends on mechanisms of tissue repair but also on the capacity of the central nervous system for compensating of permanent damage.
Objectives: We aimed to investigate changes in corticospinal plasticity and interhemispheric connections after a relapse of MS using transcranial magnetic stimulation (TMS).
Methods: Twenty healthy and 13 relapsing-remitting MS subjects with a first motor relapse were included. TMS mapping and ipsilateral silent period (iSP) were performed after relapse and at 6-month follow-up.
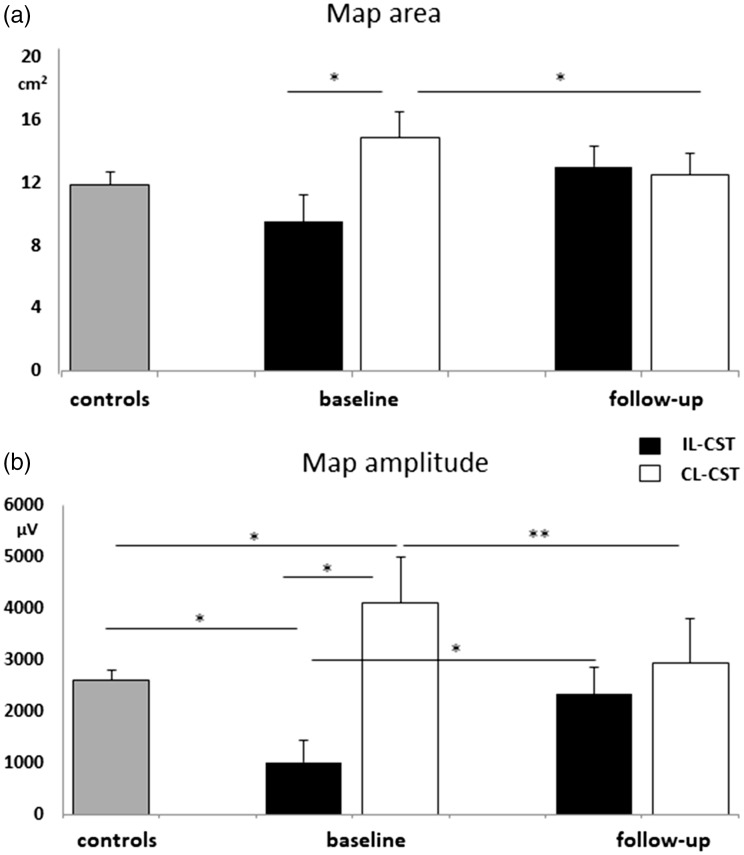
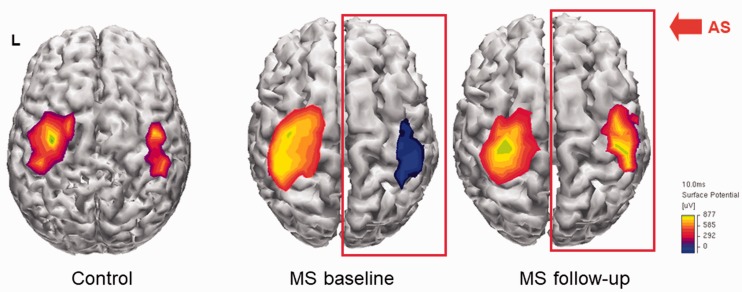
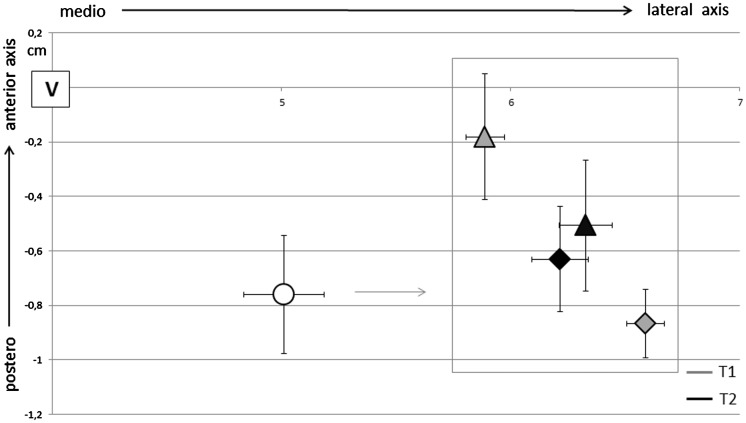
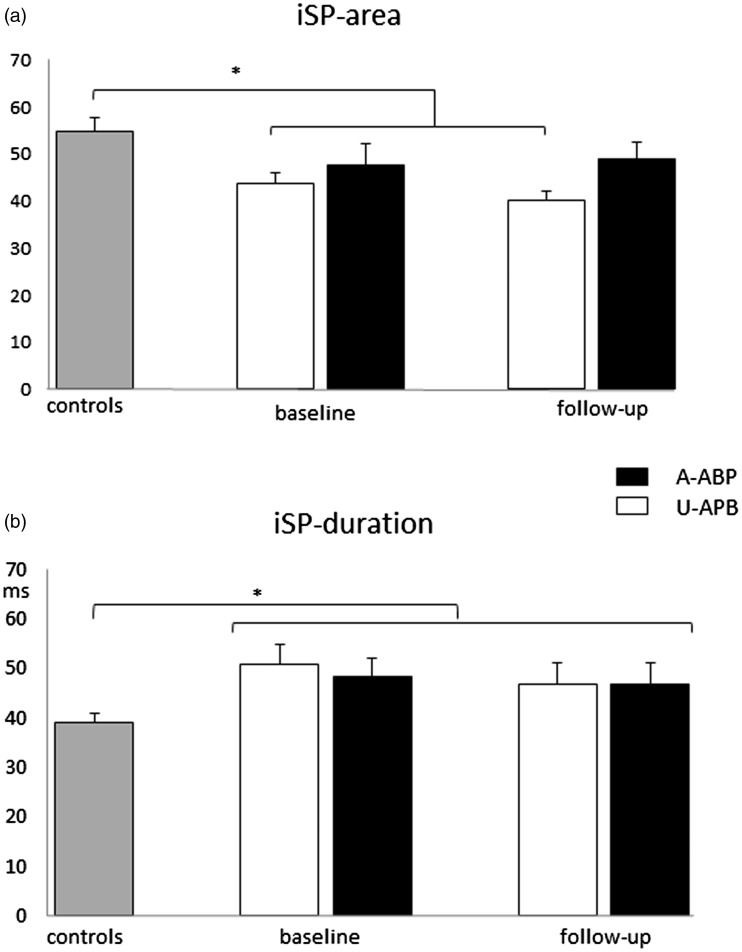
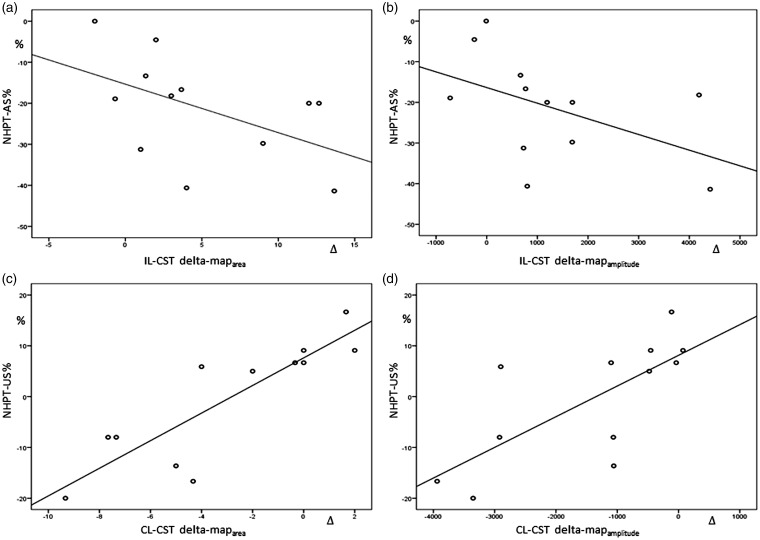
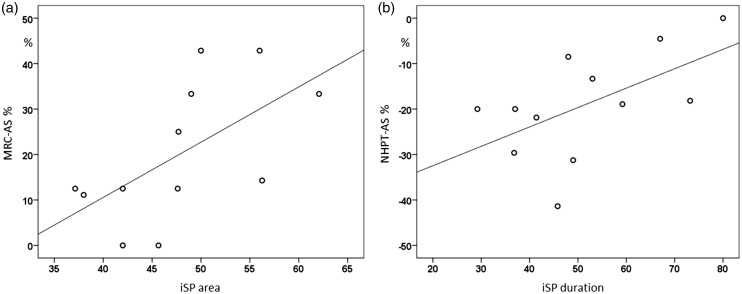
Results: Strength and dexterity of the paretic hand were impaired at baseline and improved over time. After relapse, mapamplitude and mapdensity were decreased for the ipsilesional-corticospinal tract (IL-CST) while expanded for the contralesional-CST (CL-CST). At follow-up, map parameters normalized for the CL-CST independently from recovery while the increase of outputs from the IL-CST was associated with straight and dexterity improvement. iSP measurements were impaired in MS irrespective of the phase of the disease. Prolonged iSPduration at baseline was associated with less dexterity recovery.
Conclusions: After a motor relapse, TMS mapping shows acute changes in corticospinal excitability and rearrangements of motor outputs. iSP is less influenced by the phase of disease but may better predict recovery, possibly reflecting the integrity of interhemispheric motor networks.
Keywords: TMS; iSP; mapping; multiple sclerosis; relapse.
© The Author(s) 2019.
Figures
References
-
- Filippi M, Grossman RI. MRI techniques to monitor MS evolution: The present and the future. Neurology 2002; 58(8): 1147–1153. - PubMed
-
- Filippi M, Preziosa P, Rocca MA. Brain mapping in multiple sclerosis: Lessons learned about the human brain. Neuroimage 2017; 190: 32--2. - PubMed
-
- Chieffo R, Inuggi A, Straffi L, et al. Mapping early changes of cortical motor output after subcortical stroke: A transcranial magnetic stimulation study. Brain Stimul 2013; 6(3): 322–329. - PubMed
LinkOut - more resources
Full Text Sources
