

The prognostic significance of peritumoral tertiary lymphoid structures in breast cancer
- PMID: 31598757
- PMCID: PMC11028375
- DOI: 10.1007/s00262-019-02407-8
The prognostic significance of peritumoral tertiary lymphoid structures in breast cancer
Abstract
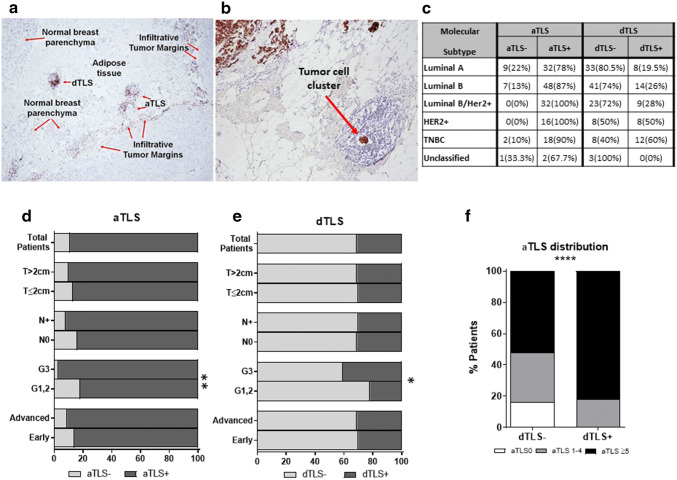
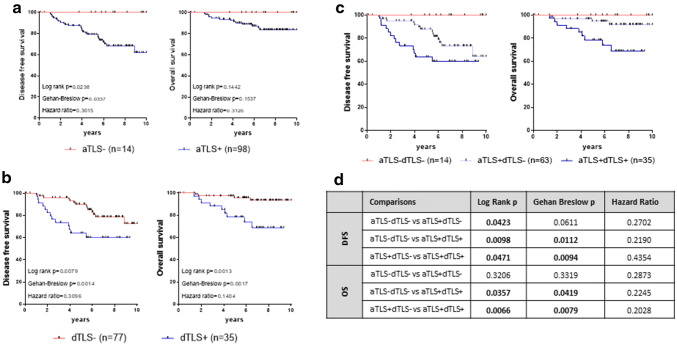
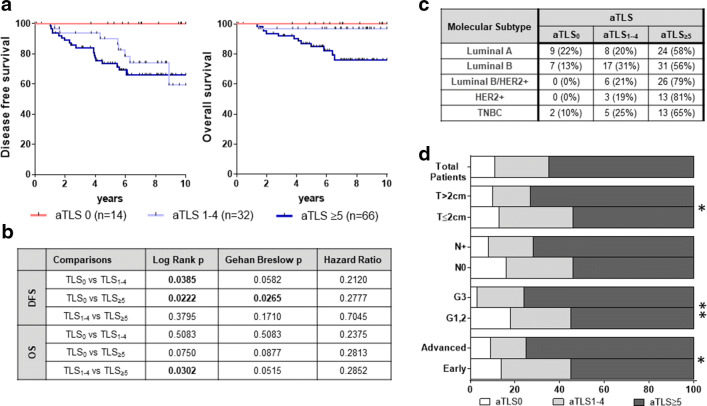
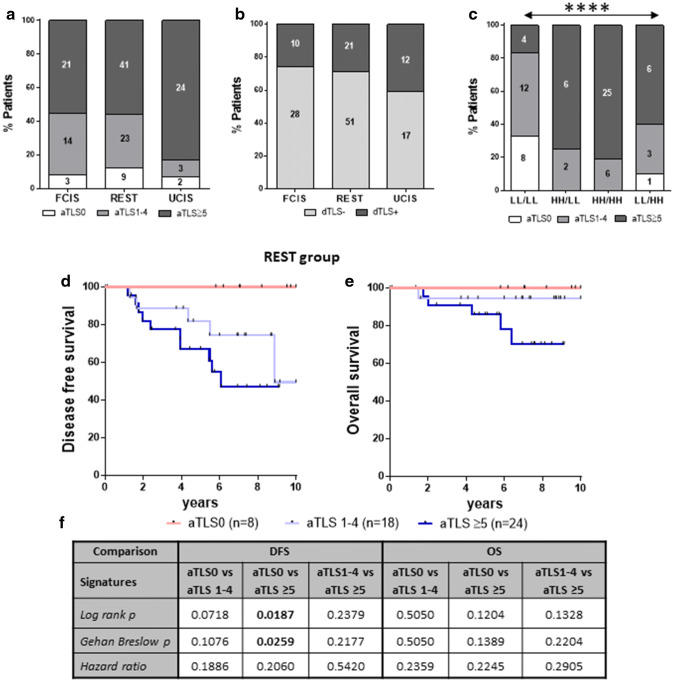
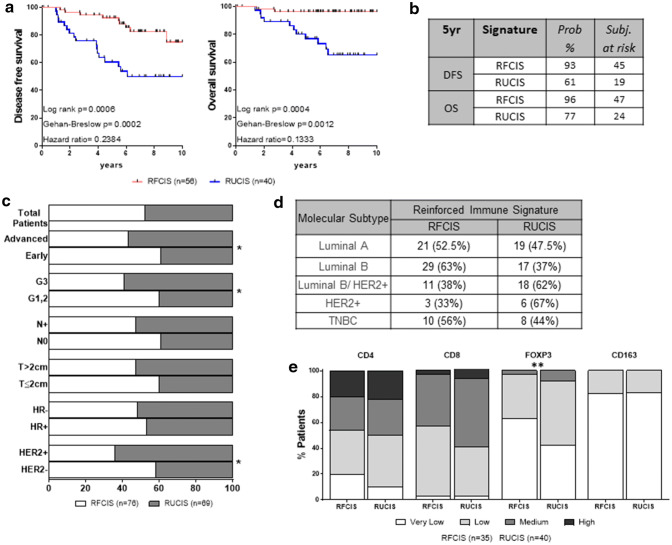
Tumors and their surrounding area represent spatially organized "ecosystems", where tumor cells and the immune contextures of the different compartments are in a dynamic interplay, with potential clinical impact. Here, we aimed to investigate the prognostic significance of peritumoral tertiary lymphoid structures (TLS) either alone or jointly with the intratumoral densities and spatial distribution of CD8 + and CD163 + cells in breast cancer (BCa) patients. TLS were identified peritumorally, within the area distancing up to 5 mm from the infiltrative tumor border, counted and further characterized as adjacent or distal, in formalin-fixed, paraffin-embedded tumor tissue samples from a cohort of 167 patients, with histologically confirmed invasive ductal BCa. TLS and tumor-infiltrating immune cells were determined by H&E and immunohistochemistry. Clinical follow-up was available for 112 of these patients. Patients with peritumoral TLS exhibited worse disease-free survival (DFS) and overall survival (OS) as compared to patients lacking TLS. Moreover, the density of peritumoral TLS was found to be crucial for prognosis, since patients with abundant TLS exhibited the worst DFS and OS. By combining the density of adjacent TLS (aTLS) with our recently published intratumoral signatures based on the differential distribution of CD8 + and CD163 + in the tumor center and invasive margin, we created two improved immune signatures with superior prognostic strength and higher patient population coverage. Our observations strengthen the notion for the fundamental role of the dynamic interplay between the immune cells within the tumor microenvironment (center/invasive margin) and the tumor surrounding area (peritumoral TLS) on the clinical outcome of BCa patients.
Keywords: Breast cancer; Immune contexture; Prognostic signatures; Tertiary lymphoid structure; Tumor infiltration.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Galluzzi L, Vacchelli E, Bravo-San Pedro JM, Buque A, Senovilla L, Baracco EE, Bloy N, Castoldi F, Abastado JP, Agostinis P, Apte RN, Aranda F, Ayyoub M, Beckhove P, Blay JY, Bracci L, Caignard A, Castelli C, Cavallo F, Celis E, Cerundolo V, Clayton A, Colombo MP, Coussens L, Dhodapkar MV, Eggermont AM, Fearon DT, Fridman WH, Fucikova J, Gabrilovich DI, Galon J, Garg A, Ghiringhelli F, Giaccone G, Gilboa E, Gnjatic S, Hoos A, Hosmalin A, Jager D, Kalinski P, Karre K, Kepp O, Kiessling R, Kirkwood JM, Klein E, Knuth A, Lewis CE, Liblau R, Lotze MT, Lugli E, Mach JP, Mattei F, Mavilio D, Melero I, Melief CJ, Mittendorf EA, Moretta L, Odunsi A, Okada H, Palucka AK, Peter ME, Pienta KJ, Porgador A, Prendergast GC, Rabinovich GA, Restifo NP, Rizvi N, Sautes-Fridman C, Schreiber H, Seliger B, Shiku H, Silva-Santos B, Smyth MJ, Speiser DE, Spisek R, Srivastava PK, Talmadge JE, Tartour E, Van Der Burg SH, Van Den Eynde BJ, Vile R, Wagner H, Weber JS, Whiteside TL, Wolchok JD, Zitvogel L, Zou W, Kroemer G. Classification of current anticancer immunotherapies. Oncotarget. 2014;5(24):12472–12508. doi: 10.18632/oncotarget.2998. - DOI - PMC - PubMed
-
- Binnewies M, Roberts EW, Kersten K, Chan V, Fearon DF, Merad M, Coussens LM, Gabrilovich DI, Ostrand-Rosenberg S, Hedrick CC, Vonderheide RH, Pittet MJ, Jain RK, Zou W, Howcroft TK, Woodhouse EC, Weinberg RA, Krummel MF. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24(5):541–550. doi: 10.1038/s41591-018-0014-x. - DOI - PMC - PubMed
-
- Keren L, Bosse M, Marquez D, Angoshtari R, Jain S, Varma S, Yang SR, Kurian A, Van Valen D, West R, Bendall SC, Angelo M. A structured tumor-immune microenvironment in triple negative breast cancer revealed by multiplexed ion beam imaging. Cell. 2018;174(6):1373–1387. doi: 10.1016/j.cell.2018.08.039. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
