

FGF23 and Associated Disorders of Phosphate Wasting
- PMID: 31599133
- PMCID: PMC7040960
- DOI: 10.17458/per.vol17.2019.gi.fgf23anddisordersphosphate
FGF23 and Associated Disorders of Phosphate Wasting
Abstract
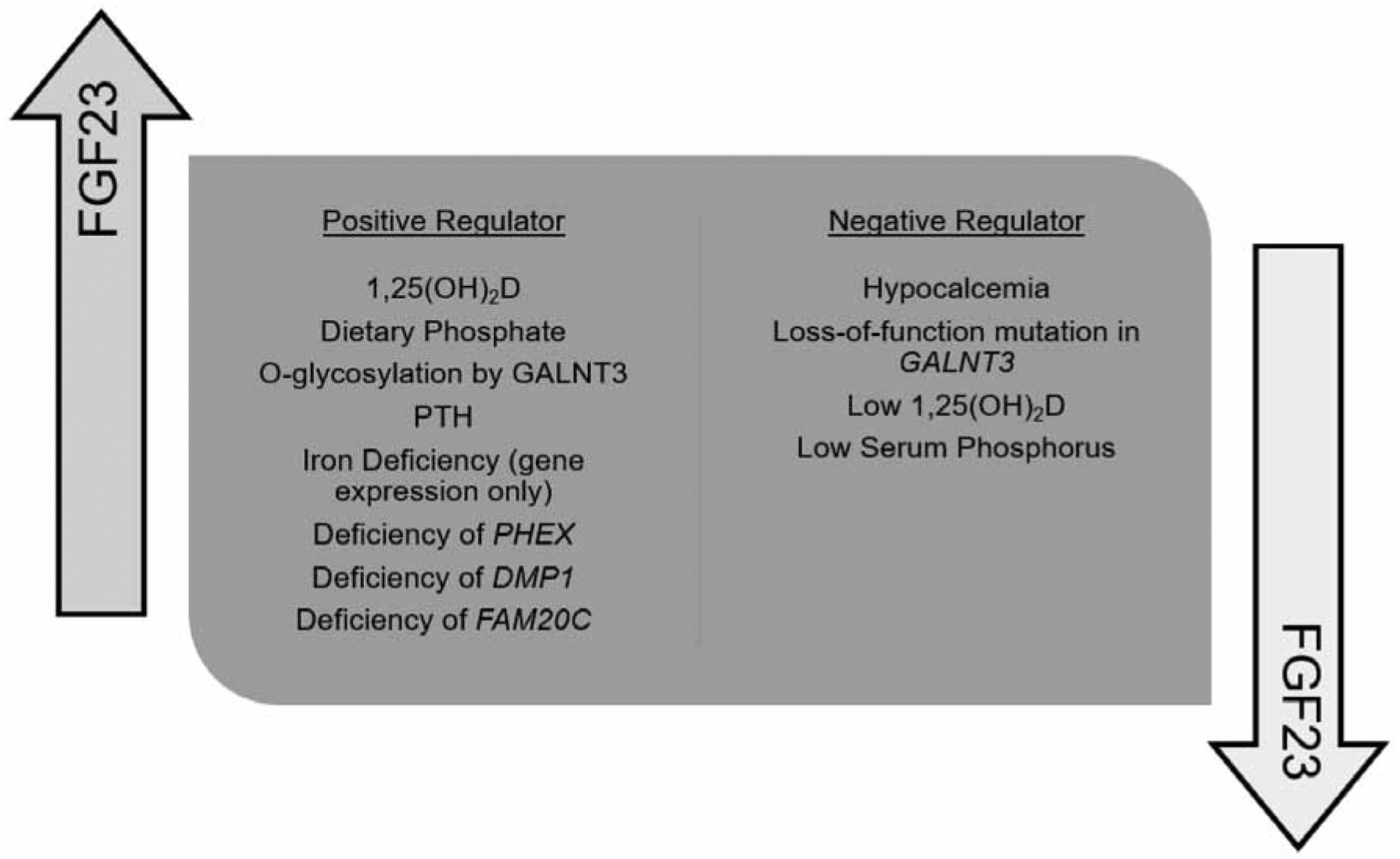
Fibroblast growth factor 23 (FGF23), one of the endocrine fibroblast growth factors, is a principal regulator in the maintenance of serum phosphorus concentration. Binding to its cofactor αKlotho and a fibroblast growth factor receptor is essential for its activity. Its regulation and interaction with other factors in the bone-parathyroid-kidney axis is complex. FGF23 reduces serum phosphorus concentration through decreased reabsorption of phosphorus in the kidney and by decreasing 1,25 dihydroxyvitamin D (1,25(OH)2D) concentrations. Various FGF23-mediated disorders of renal phosphate wasting share similar clinical and biochemical features. The most common of these is X-linked hypophosphatemia (XLH). Additional disorders of FGF23 excess include autosomal dominant hypophosphatemic rickets, autosomal recessive hypophosphatemic rickets, fibrous dysplasia, and tumor-induced osteomalacia. Treatment is challenging, requiring careful monitoring and titration of dosages to optimize effectiveness and to balance side effects. Conventional therapy for XLH and other disorders of FGF23-mediated hypophosphatemia involves multiple daily doses of oral phosphate salts and active vitamin D analogs, such as calcitriol or alfacalcidol. Additional treatments may be used to help address side effects of conventional therapy such as thiazides to address hypercalciuria or nephrocalcinosis, and calcimimetics to manage hyperparathyroidism. The recent development and approval of an anti-FGF23 antibody, burosumab, for use in XLH provides a novel treatment option.
Keywords: 1,25(OH)2D; Burosumab; FGF23; Klotho; Phosphorus; Rickets; XLH.
Copyright© of YS Medical Media ltd.
Figures

References
-
- Yayon A, Klagsbrun M, Esko JD, Leder P, Ornitz DM. Cell surface, heparin-like molecules are required for binding of basic fibroblast growth factor to its high affinity receptor. Cell 1991;64(4):841–848 - PubMed
-
- Liu S, Quarles LD. How fibroblast growth factor 23 works. Journal of the American Society of Nephrology 2007;18(6):1637–1647 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources