

A sarcoidosis-lymphoma syndrome revealed by hypopituitarism
- PMID: 31600729
- PMCID: PMC6765315
- DOI: 10.1530/EDM-19-0091
A sarcoidosis-lymphoma syndrome revealed by hypopituitarism
Abstract
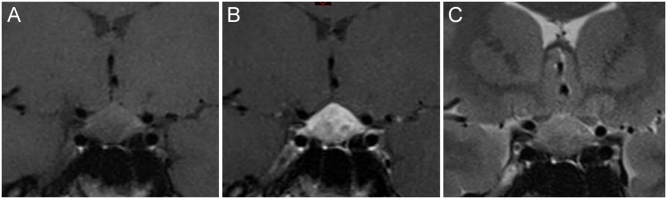
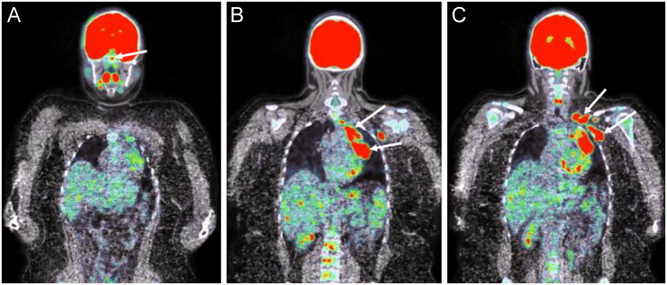
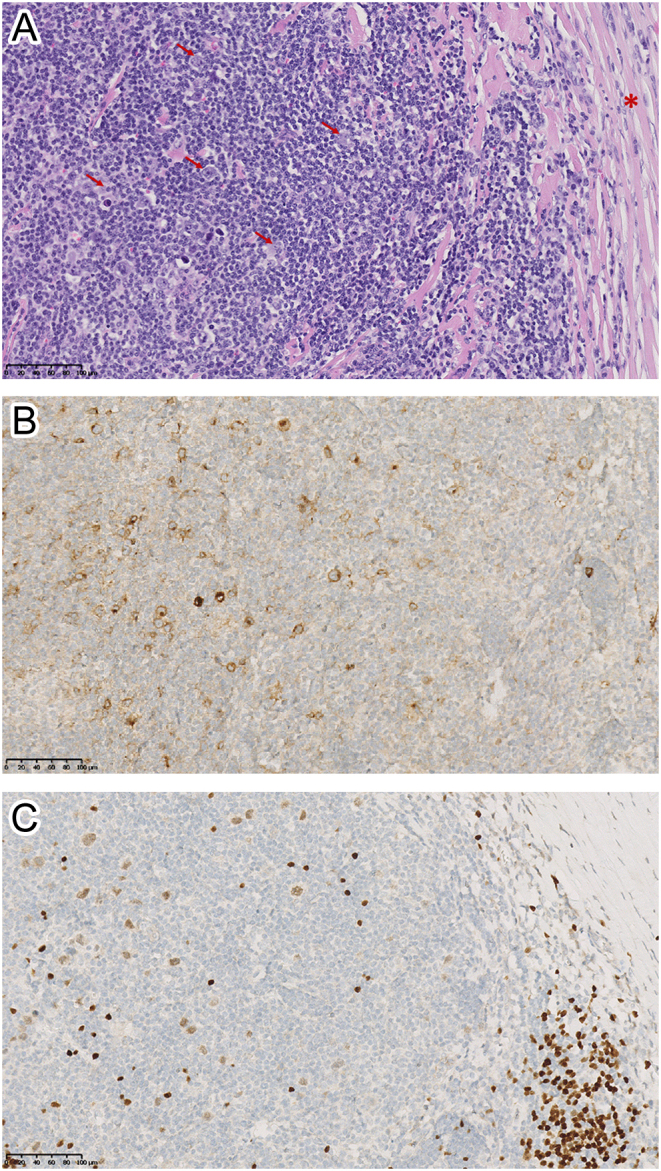
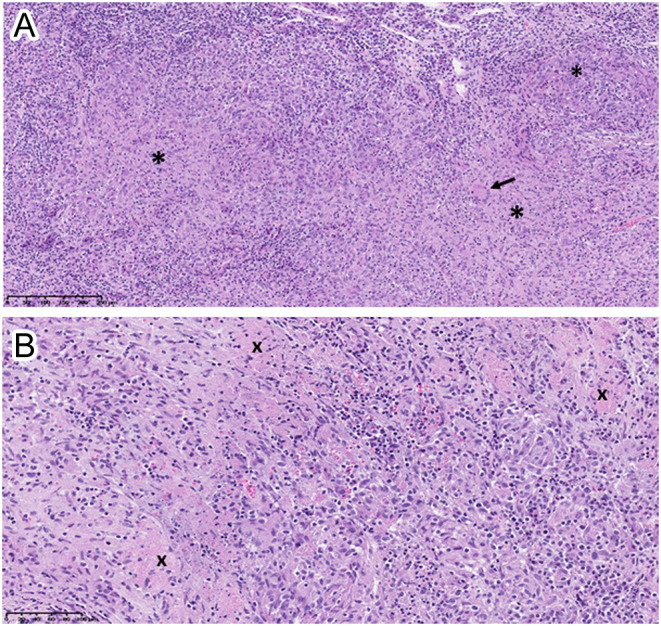
Summary: A 26-year-old woman presented with persistent headache and tiredness. Biological investigations disclosed a moderate inflammatory syndrome, low PTH-hypercalcemia and complete anterior hypopituitarism. A magnetic resonance imaging (MRI) of the pituitary gland was performed and revealed a symmetric enlargement with a heterogeneous signal. Ophthalmological examination showed an asymptomatic bilateral anterior and posterior uveitis, and a diagnosis of pituitary sarcoidosis was suspected. As the localization of lymphadenopathies on the fused whole-body FDG-PET/computerized tomography (CT) was not evoking a sarcoidosis in first instance, an excisional biopsy of a left supraclavicular adenopathy was performed showing classic nodular sclerosis Hodgkin's lymphoma (HL). A diagnostic transsphenoidal biopsy of the pituitary gland was proposed for accurate staging of the HL and surprisingly revealed typical granulomatous inflammation secondary to sarcoidosis, leading to the diagnosis of a sarcoidosis-lymphoma syndrome. The co-existence of these diseases constitutes a diagnostic challenge and we emphasize the necessity of exact staging of disease in order to prescribe adequate treatment.
Learning points: The possibility of a sarcoidosis-lymphoma syndrome, although rare, should be kept in mind during evaluation for lymphadenopathies. In the case of such association, lymphoma usually occurs after sarcoidosis. However, sarcoidosis and lymphoma can be detected simultaneously and development of sarcoidosis in a patient with previous lymphoma has also been reported. An accurate diagnosis of the disease and the respective organ involvements, including biopsy, is necessary in order to prescribe adequate treatment.
Keywords: 2019; 25-hydroxyvitamin-D3; ACTH; Adolescent/young adult; Belgium; C-reactive protein; CT scan; Chemotherapy; Cortisol; Cortisol (9am); Dacarbazine; FSH; FT4; Fatigue; Female; General practice; Glucocorticoids; Haematoxylin and eosin staining; Headache; Histopathology; Hydrocortisone; Hypercalcaemia; Hypopituitarism; IGF1; Immunohistochemistry; LH; Levothyroxine; Lymphadenitis; Lymphadenopathy; MRI; Methylprednisolone; New disease or syndrome: presentations/diagnosis/management; PET scan; PTH; Pituitary; Sarcoidosis; September; TSH; Thyroxine (T4); White; X-ray.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
