

Phenotyping diabetic cardiomyopathy in Europeans and South Asians
- PMID: 31604432
- PMCID: PMC6788052
- DOI: 10.1186/s12933-019-0940-z
Phenotyping diabetic cardiomyopathy in Europeans and South Asians
Abstract
Background: The pathogenesis and cardiovascular impact of type 2 diabetes (T2D) may be different in South Asians compared with other ethnic groups. The phenotypic characterization of diabetic cardiomyopathy remains debated and little is known regarding differences in T2D-related cardiovascular remodeling across ethnicities. We aimed to characterize the differences in left ventricular (LV) diastolic and systolic function, LV structure, myocardial tissue characteristics and aortic stiffness between T2D patients and controls and to assess the differences in T2D-related cardiovascular remodeling between South Asians and Europeans.
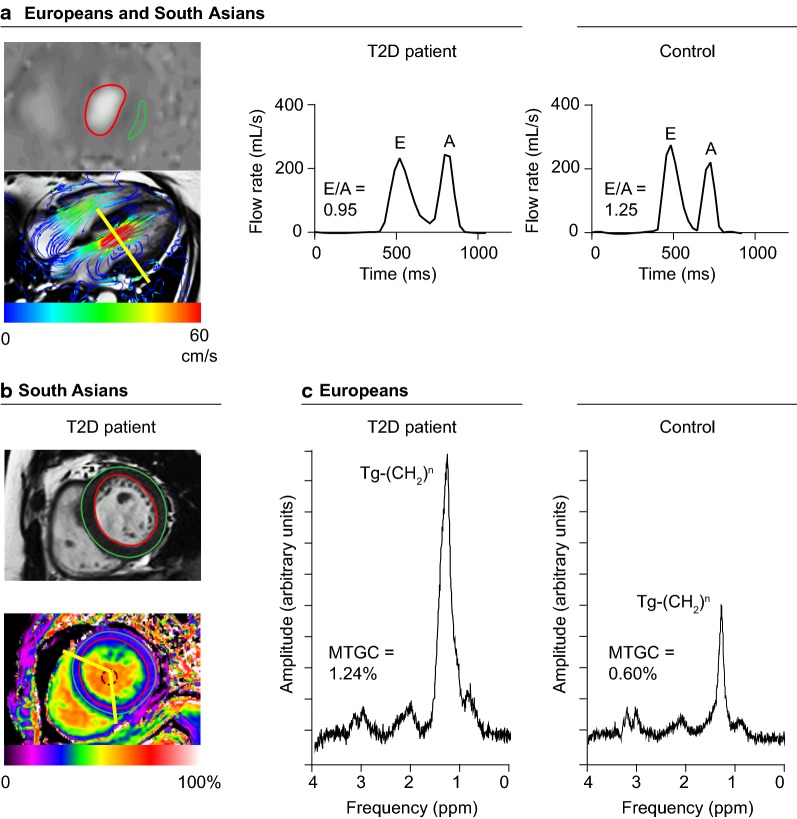
Methods: T2D patients and controls of South Asian and European descent underwent 3 Tesla cardiovascular magnetic resonance imaging (CMR) and cardiac proton-magnetic resonance spectroscopy (1H-MRS). Differences in cardiovascular parameters between T2D patients and controls were examined using ANCOVA and were reported as mean (95% CI). Ethnic group comparisons in the association of T2D with cardiovascular remodeling were made by adding the interaction term between ethnicity and diabetes status to the model.
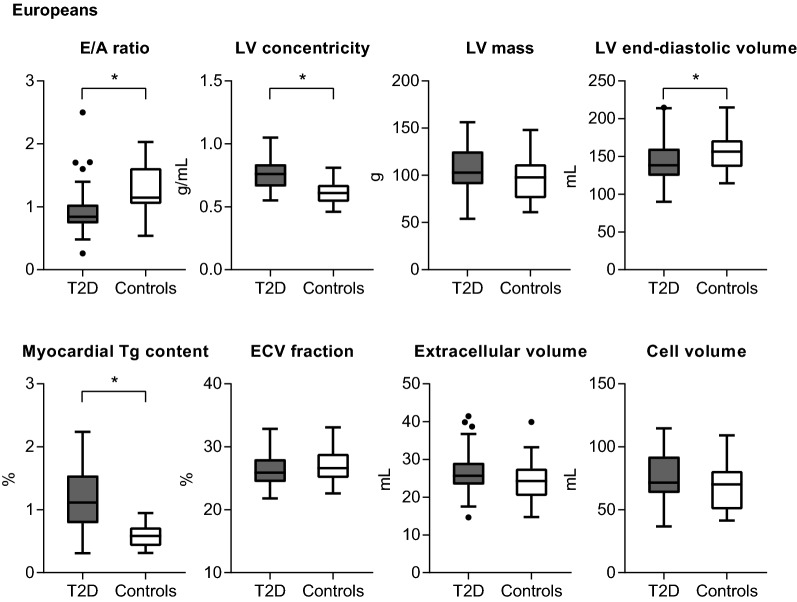
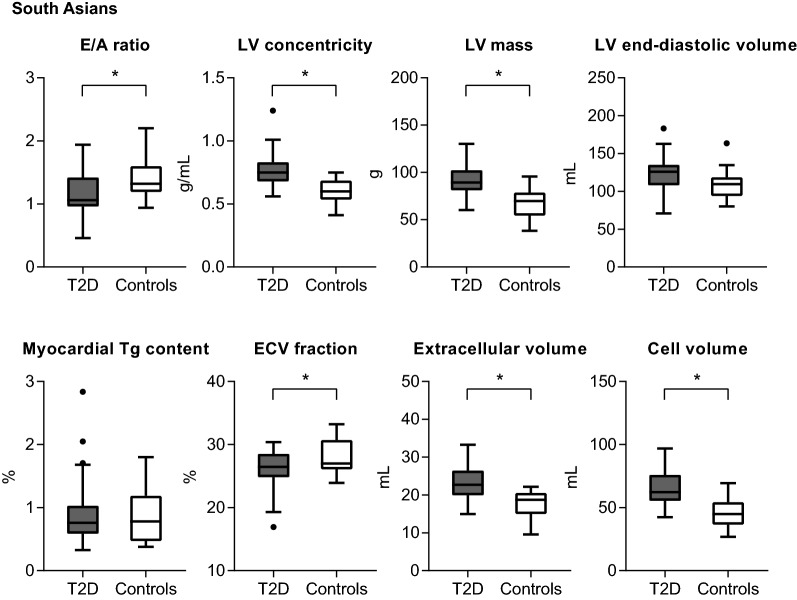
Results: A total of 131 individuals were included (54 South Asians [50.1 ± 8.7 years, 33% men, 33 patients vs. 21 controls) and 77 Europeans (58.8 ± 7.0 years, 56% men, 48 patients vs. 29 controls)]. The ratio of the transmitral early and late peak filling rate (E/A) was lower in T2D patients compared with controls, in South Asians [- 0.20 (- 0.36; - 0.03), P = 0.021] and Europeans [- 0.20 (- 0.36; - 0.04), P = 0.017], whereas global longitudinal strain and aortic pulse wave velocity were similar. South Asian T2D patients had a higher LV mass [+ 22 g (15; 30), P < 0.001] (P for interaction by ethnicity = 0.005) with a lower extracellular volume fraction [- 1.9% (- 3.4; - 0.4), P = 0.013] (P for interaction = 0.114), whilst European T2D patients had a higher myocardial triglyceride content [+ 0.59% (0.35; 0.84), P = 0.001] (P for interaction = 0.002) than their control group.
Conclusions: Diabetic cardiomyopathy was characterized by impaired LV diastolic function in South Asians and Europeans. Increased LV mass was solely observed among South Asian T2D patients, whereas differences in myocardial triglyceride content between T2D patients and controls were only present in the European cohort. The diabetic cardiomyopathy phenotype may differ between subsets of T2D patients, for example across ethnicities, and tailored strategies for T2D management may be required.
Keywords: Diabetes mellitus, type 2; Diabetic cardiomyopathies; European; Myocardial diffuse fibrosis; Myocardial steatosis; Proton-magnetic resonance spectroscopy; South Asian; T1 mapping.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tillin T, Hughes AD, Mayet J, Whincup P, Sattar N, Forouhi NG, et al. The relationship between metabolic risk factors and incident cardiovascular disease in Europeans, South Asians, and African Caribbeans: SABRE (Southall and Brent Revisited)—a prospective population-based study. J Am Coll Cardiol. 2013;61(17):1777–1786. doi: 10.1016/j.jacc.2012.12.046. - DOI - PMC - PubMed
-
- Kanaya AM, Wassel CL, Mathur D, Stewart A, Herrington D, Budoff MJ, et al. Prevalence and correlates of diabetes in South Asian Indians in the United States: findings from the metabolic syndrome and atherosclerosis in South Asians living in America study and the multi-ethnic study of atherosclerosis. Metab Syndr Relat Disord. 2010;8(2):157–164. doi: 10.1089/met.2009.0062. - DOI - PMC - PubMed
-
- Gujral UP, Vittinghoff E, Mongraw-Chaffin M, Vaidya D, Kandula NR, Allison M, et al. Cardiometabolic abnormalities among normal-weight persons from five racial/ethnic groups in the United States: a cross-sectional analysis of two cohort studies. Ann Intern Med. 2017;166(9):628–636. doi: 10.7326/M16-1895. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
