

Frequency of Screening and SBT Technique Trial - North American Weaning Collaboration (FAST-NAWC): a protocol for a multicenter, factorial randomized trial
- PMID: 31604480
- PMCID: PMC6787986
- DOI: 10.1186/s13063-019-3641-8
Frequency of Screening and SBT Technique Trial - North American Weaning Collaboration (FAST-NAWC): a protocol for a multicenter, factorial randomized trial
Abstract
Rationale: In critically ill patients receiving invasive mechanical ventilation (MV), research supports the use of daily screening to identify patients who are ready to undergo a spontaneous breathing trial (SBT) followed by conduct of an SBT. However, once daily (OD) screening is poorly aligned with the continuous care provided in most intensive care units (ICUs) and the best SBT technique for clinicians to use remains controversial.
Objectives: To identify the optimal screening frequency and SBT technique to wean critically ill adults in the ICU.
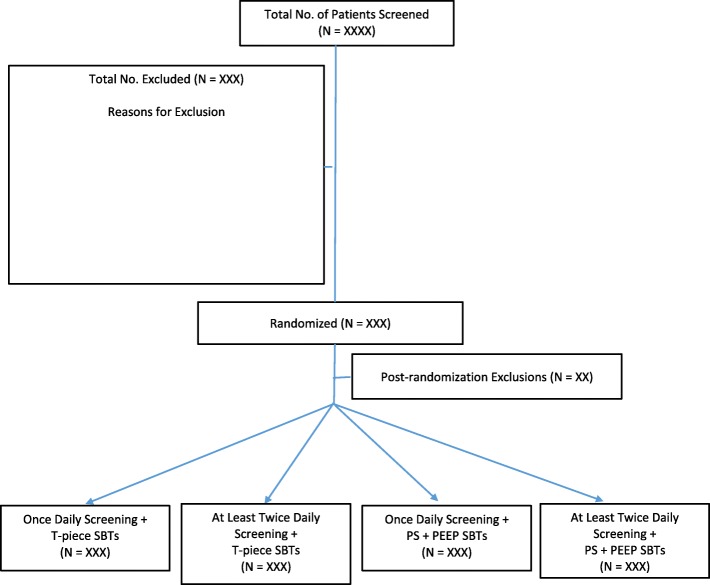
Methods: We aim to conduct a multicenter, factorial design randomized controlled trial with concealed allocation, comparing the effect of both screening frequency (once versus at least twice daily [ALTD]) and SBT technique (Pressure Support [PS] + Positive End-Expiratory Pressure [PEEP] vs T-piece) on the time to successful extubation (primary outcome) in 760 critically ill adults who are invasively ventilated for at least 24 h in 20 North American ICUs. In the OD arm, respiratory therapists (RTs) will screen study patients between 06:00 and 08:00 h. In the ALTD arm, patients will be screened at least twice daily between 06:00 and 08:00 h and between 13:00 and 15:00 h with additional screens permitted at the clinician's discretion. When the SBT screen is passed, an SBT will be conducted using the assigned technique (PS + PEEP or T-piece). We will follow patients until successful extubation, death, ICU discharge, or until day 60 after randomization. We will contact patients or their surrogates six months after randomization to assess health-related quality of life and functional status.
Relevance: The around-the-clock availability of RTs in North American ICUs presents an important opportunity to identify the optimal SBT screening frequency and SBT technique to minimize patients' exposure to invasive ventilation and ventilator-related complications.
Trial registration: Clinical Trials.gov, NCT02399267 . Registered on Nov 21, 2016 first registered.
Keywords: Randomized controlled trial; Screening; Spontaneous breathing trial; Successful extubation; Weaning.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Heyland DK, Cook DJ, Griffith L, Keenan SP, Brun-Buisson C. The attributable morbidity and mortality of ventilator associated pneumonia in the critically ill patient. The Canadian Critical Care Trials Group. Am J Respir Crit Care Med. 1999;159:1249–1256. doi: 10.1164/ajrccm.159.4.9807050. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
