

Nodular Leptomeningeal Disease-A Distinct Pattern of Recurrence After Postresection Stereotactic Radiosurgery for Brain Metastases: A Multi-institutional Study of Interobserver Reliability
- PMID: 31605786
- PMCID: PMC9527087
- DOI: 10.1016/j.ijrobp.2019.10.002
Nodular Leptomeningeal Disease-A Distinct Pattern of Recurrence After Postresection Stereotactic Radiosurgery for Brain Metastases: A Multi-institutional Study of Interobserver Reliability
Abstract
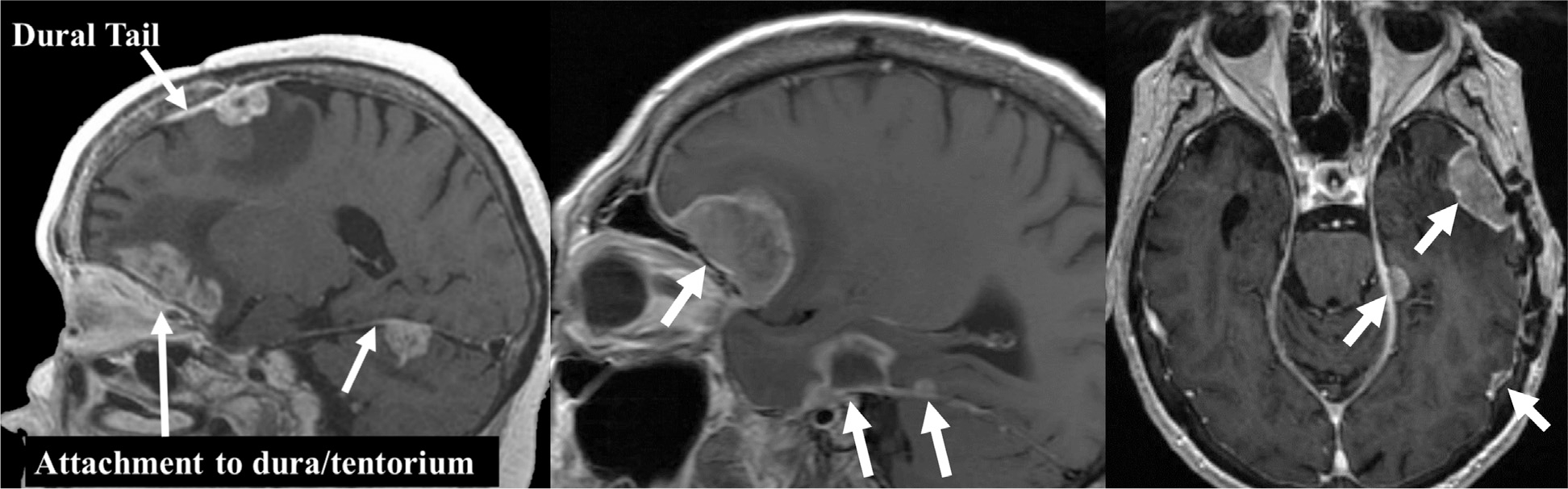
Purpose: For brain metastases, surgical resection with postoperative stereotactic radiosurgery is an emerging standard of care. Postoperative cavity stereotactic radiosurgery is associated with a specific, underrecognized pattern of intracranial recurrence, herein termed nodular leptomeningeal disease (nLMD), which is distinct from classical leptomeningeal disease. We hypothesized that there is poor consensus regarding the definition of LMD, and that a formal, self-guided training module will improve interrater reliability (IRR) and validity in diagnosing LMD.
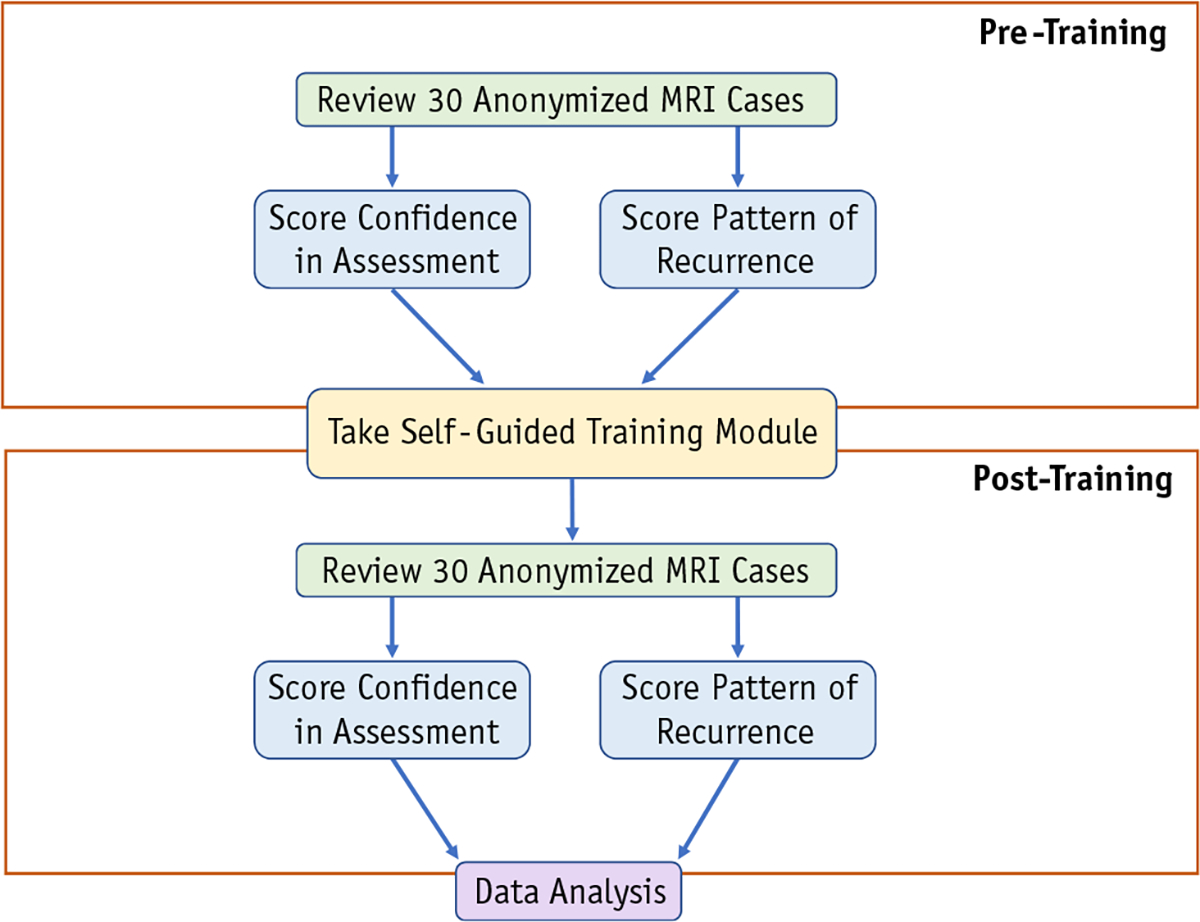
Methods and materials: Twenty-two physicians at 16 institutions, including 15 physicians with central nervous system expertise, completed a 2-phase survey that included magnetic resonance imaging and treatment information for 30 patients. In the "pretraining" phase, physicians labeled cases using 3 patterns of recurrence commonly reported in prospective studies: local recurrence (LR), distant parenchymal recurrence (DR), and LMD. After a self-directed training module, participating physicians completed the "posttraining" phase and relabeled the 30 cases using the 4 following labels: LR, DR, classical leptomeningeal disease, and nLMD.
Results: IRR increased 34% after training (Fleiss' Kappa K = 0.41 to K = 0.55, P < .001). IRR increased most among non-central nervous system specialists (+58%, P < .001). Before training, IRR was lowest for LMD (K = 0.33). After training, IRR increased across all recurrence subgroups and increased most for LMD (+67%). After training, ≥27% of cases initially labeled LR or DR were later recognized as nLMD.
Conclusions: This study highlights the large degree of inconsistency among clinicians in recognizing nLMD. Our findings demonstrate that a brief self-guided training module distinguishing nLMD can significantly improve IRR across all patterns of recurrence, and particularly in nLMD. To optimize outcomes reporting, prospective trials in brain metastases should incorporate central imaging review and investigator training.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Classifying Leptomeningeal Disease: An Essential Element in Managing Advanced Metastatic Disease in the Central Nervous System.Int J Radiat Oncol Biol Phys. 2020 Mar 1;106(3):587-588. doi: 10.1016/j.ijrobp.2019.12.016. Int J Radiat Oncol Biol Phys. 2020. PMID: 32014150 No abstract available.
References
-
- Ostrom QT, Wright CH, Barnholtz-Sloan JS. Brain metastases: Epidemiology. Handb Clin Neurol 2018;149:27–42. - PubMed
-
- Armstrong JG, Wronski M, Galicich J, Arbit E, Leibel SA, Burt M. Postoperative radiation for lung cancer metastatic to the brain. J Clin Oncol 1994;12:2340–2344. - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases. JAMA 2006;295:2483. - PubMed
-
- Soltys SG, Adler JR, Lipani JD, et al. Stereotactic radiosurgery of the postoperative resection cavity for brain metastases. Int J Radiat Oncol 2008;70:187–193. - PubMed
-
- Iwai Y, Yamanaka K, Yasui T. Boost radiosurgery for treatment of brain metastases after surgical resections. Surg Neurol 2008;69:181–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
