

Hepcidin-guided screen-and-treat interventions against iron-deficiency anaemia in pregnancy: a randomised controlled trial in The Gambia
- PMID: 31607468
- PMCID: PMC7109523
- DOI: 10.1016/S2214-109X(19)30393-6
Hepcidin-guided screen-and-treat interventions against iron-deficiency anaemia in pregnancy: a randomised controlled trial in The Gambia
Abstract
Background: WHO recommends daily iron supplementation for pregnant women, but adherence is poor because of side-effects, effectiveness is low, and there are concerns about possible harm. The iron-regulatory hormone hepcidin can signal when an individual is ready-and-safe to receive iron. We tested whether a hepcidin-guided screen-and-treat approach to combat iron-deficiency anaemia could achieve equivalent efficacy to universal administration, but with lower exposure to iron.
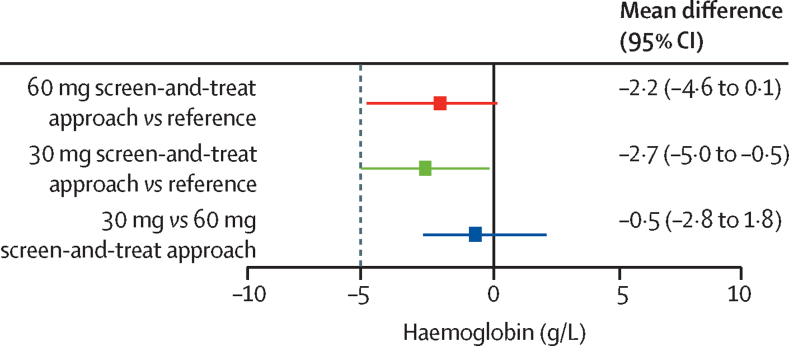
Methods: We did a three-arm, randomised, double-blind, non-inferiority trial in 19 rural communities in the Jarra West and Kiang East districts of The Gambia. Eligible participants were pregnant women aged 18-45 years at between 14 weeks and 22 weeks of gestation. We randomly allocated women to either WHO's recommended regimen (ie, a daily UN University, UNICEF, and WHO international multiple-micronutrient preparation [UNIMMAP] containing 60 mg iron), a 60 mg screen-and-treat approach (ie, daily UNIMMAP containing 60 mg iron for 7 days if weekly hepcidin was <2·5 μg/L or UNIMMAP without iron if hepcidin was ≥2·5 μg/L), or a 30 mg screen-and-treat approach (ie, daily UNIMMAP containing 30 mg iron for 7 days if weekly hepcidin was <2·5 μg/L or UNIMMAP without iron if hepcidin was ≥2·5 μg/L). We used a block design stratified by amount of haemoglobin at enrolment (above and below the median amount of haemoglobin on every enrolment day) and stage of gestation (14-18 weeks vs 19-22 weeks). Participants and investigators were unaware of the random allocation. The primary outcome was the amount of haemoglobin at day 84 and was measured as the difference in haemoglobin in each screen-and-treat group compared with WHO's recommended regimen; the non-inferiority margin was set at -5·0 g/L. The primary outcome was assessed in the per-protocol population, which comprised all women who completed the study. This trial is registered with the ISRCTN registry, number ISRCTN21955180.
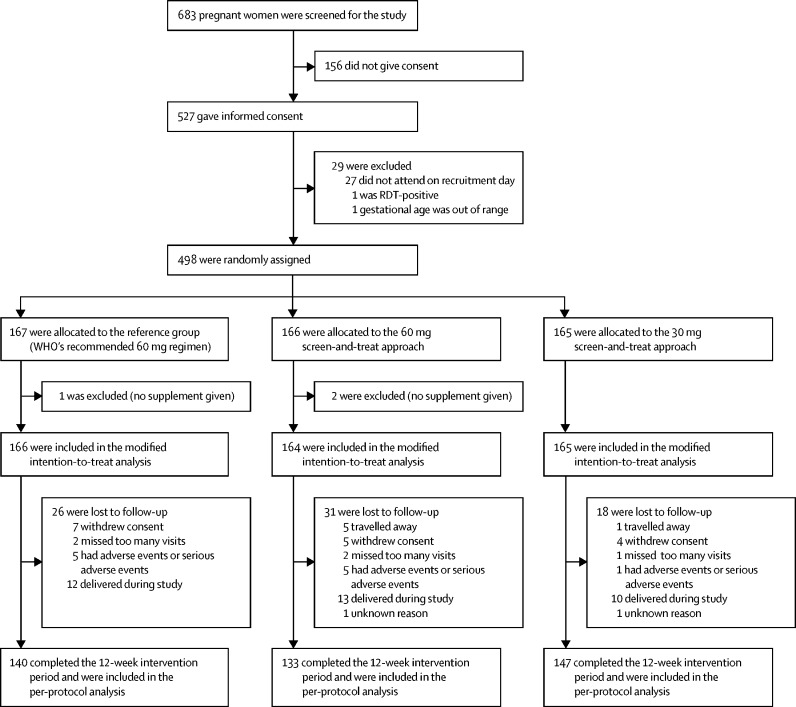
Findings: Between June 16, 2014, and March 3, 2016, 498 participants were randomised, of whom 167 were allocated to WHO's recommended regimen, 166 were allocated to the 60 mg per day screen-and-treat approach, and 165 were allocated to the 30 mg per day screen-and-treat approach. 78 participants were withdrawn or lost to follow-up during the study; thus, the per-protocol population comprised 140 women assigned to WHO's recommended regimen, 133 allocated to the 60 mg screen-and-treat approach, and 147 allocated to the 30 mg screen-and-treat approach. The screen-and-treat approaches did not exceed the non-inferiority margin. Compared with WHO's recommended regimen, the difference in the amount of haemoglobin at day 84 was -2·2 g/L (95% CI -4·6 to 0·1) with the 60 mg screen-and-treat approach and -2·7 g/L (-5·0 to -0·5) with the 30 mg screen-and-treat approach. Adherence, reported side-effects, and adverse events were similar between the three groups. The most frequent side-effect was stomachache, which was similar in the 60 mg screen-and-treat group (82 cases per 1906 person-weeks) and with WHO's recommended regimen (81 cases per 1974 person-weeks; effect 1·0, 95% CI 0·7 to 1·6); in the 30 mg screen-and-treat group the frequency of stomachache was slightly lower than with WHO's recommended regimen (58 cases per 2009 person-weeks; effect 0·7, 95% CI 0·5 to 1·1). No participants died during the study.
Interpretation: The hepcidin-guided screen-and-treat approaches had no advantages over WHO's recommended regimen in terms of adherence, side-effects, or safety outcomes. Our results suggest that the current WHO policy for iron administration to pregnant women should remain unchanged while more effective approaches continue to be sought.
Funding: Bill & Melinda Gates Foundation and the UK Medical Research Council.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Iron-deficiency anaemia in pregnancy: the role of hepcidin.Lancet Glob Health. 2019 Nov;7(11):e1476-e1477. doi: 10.1016/S2214-109X(19)30414-0. Lancet Glob Health. 2019. PMID: 31607452 No abstract available.
References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. - PMC - PubMed
-
- WHO e-Library of Evidence for Nutrition Actions (eLENA): daily iron and folic acid supplementation during pregnancy. Feb 11, 2019. http://www.who.int/elena/titles/daily_iron_pregnancy/en/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
