

Feasibility, Safety, and Outcome of Endovascular Recanalization in Childhood Stroke: The Save ChildS Study
- PMID: 31609380
- PMCID: PMC6802048
- DOI: 10.1001/jamaneurol.2019.3403
Feasibility, Safety, and Outcome of Endovascular Recanalization in Childhood Stroke: The Save ChildS Study
Abstract
Importance: Randomized clinical trials have shown the efficacy of thrombectomy of large intracranial vessel occlusions in adults; however, any association of therapy with clinical outcomes in children is unknown.
Objective: To evaluate the use of endovascular recanalization in pediatric patients with arterial ischemic stroke.
Design, setting, and participants: This retrospective, multicenter cohort study, conducted from January 1, 2000, to December 31, 2018, analyzed the databases from 27 stroke centers in Europe and the United States. Included were all pediatric patients (<18 years) with ischemic stroke who underwent endovascular recanalization. Median follow-up time was 16 months.
Exposures: Endovascular recanalization.
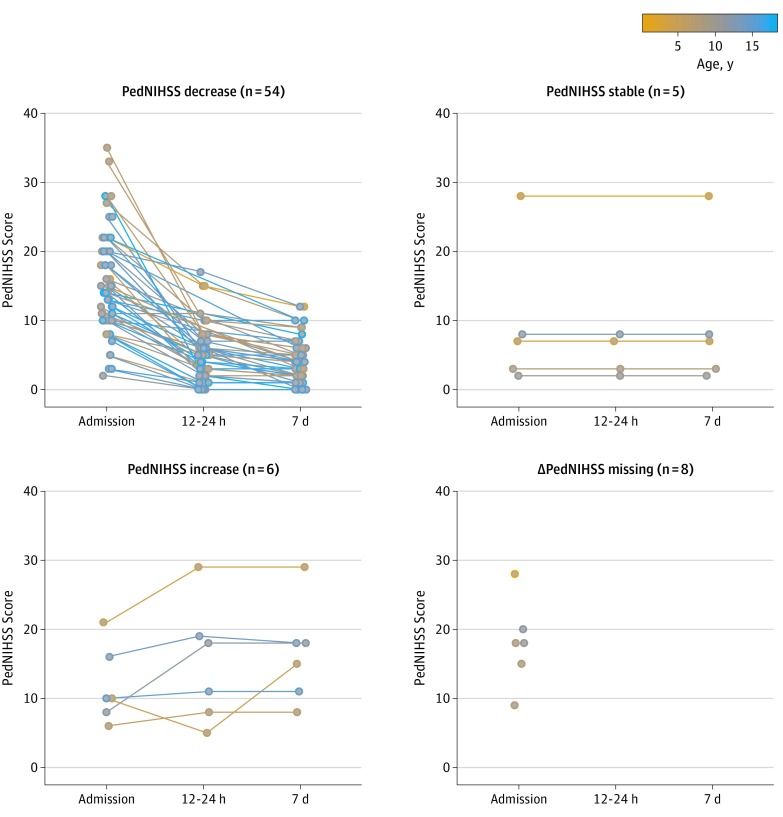
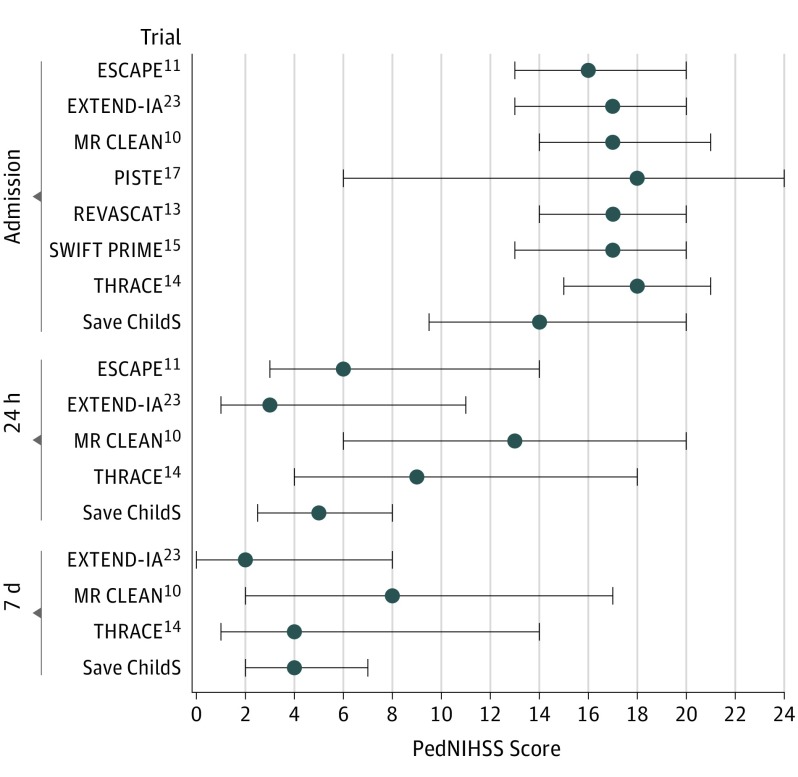
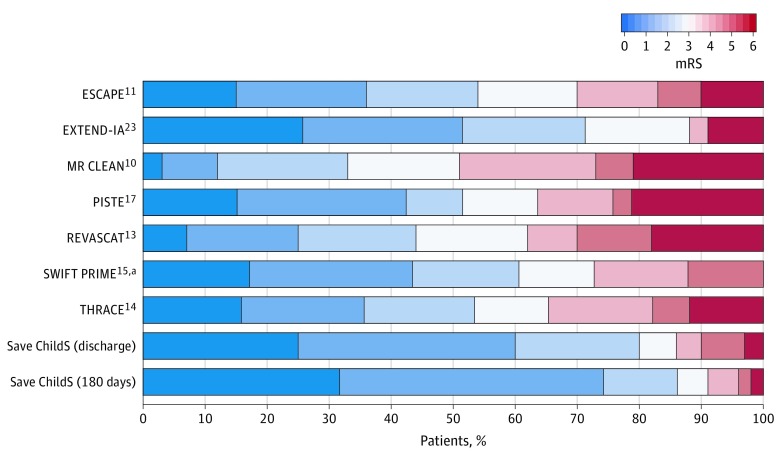
Main outcomes and measures: The decrease of the Pediatric National Institutes of Health Stroke Scale (PedNIHSS) score from admission to day 7 was the primary outcome (score range: 0 [no deficit] to 34 [maximum deficit]). Secondary clinical outcomes included the modified Rankin scale (mRS) (score range: 0 [no deficit] to 6 [death]) at 6 and 24 months and rate of complications.
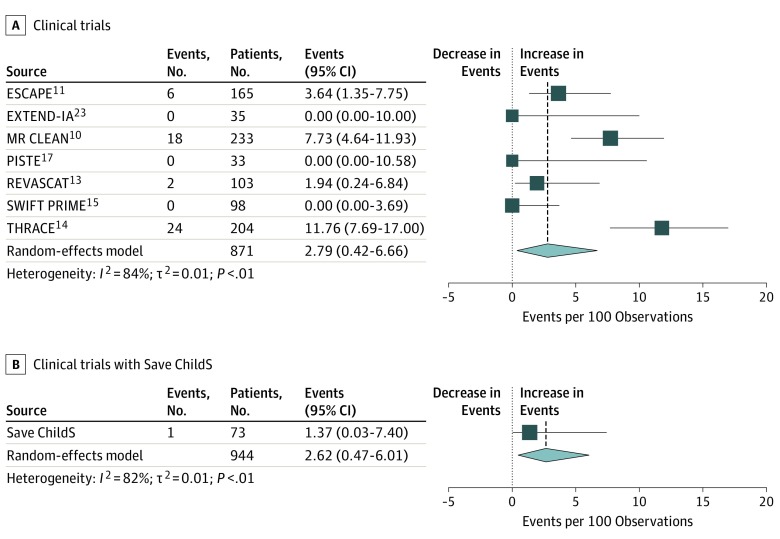
Results: Seventy-three children from 27 participating stroke centers were included. Median age was 11.3 years (interquartile range [IQR], 7.0-15.0); 37 patients (51%) were boys, and 36 patients (49%) were girls. Sixty-three children (86%) received treatment for anterior circulation occlusion and 10 patients (14%) received treatment for posterior circulation occlusion; 16 patients (22%) received concomitant intravenous thrombolysis. Neurologic outcome improved from a median PedNIHSS score of 14.0 (IQR, 9.2-20.0) at admission to 4.0 (IQR, 2.0-7.3) at day 7. Median mRS score was 1.0 (IQR, 0-1.6) at 6 months and 1.0 (IQR, 0-1.0) at 24 months. One patient (1%) developed a postinterventional bleeding complication and 4 patients (5%) developed transient peri-interventional vasospasm. The proportion of symptomatic intracerebral hemorrhage events in the HERMES meta-analysis of trials with adults was 2.79 (95% CI, 0.42-6.66) and in Save ChildS was 1.37 (95% CI, 0.03-7.40).
Conclusions and relevance: The results of this study suggest that the safety profile of thrombectomy in childhood stroke does not differ from the safety profile in randomized clinical trials for adults; most of the treated children had favorable neurologic outcomes. This study may support clinicians' practice of off-label thrombectomy in childhood stroke in the absence of high-level evidence.
Conflict of interest statement
Figures
Comment in
-
Endovascular Therapy for Childhood Stroke-Working Together to Reach Prime Time.JAMA Neurol. 2020 Jan 1;77(1):13-15. doi: 10.1001/jamaneurol.2019.3412. JAMA Neurol. 2020. PMID: 31609381 No abstract available.
-
Pediatric ischemic stroke.J Neurol. 2020 Apr;267(4):1221-1222. doi: 10.1007/s00415-020-09779-3. J Neurol. 2020. PMID: 32157384 No abstract available.
References
-
- Goldenberg NA, Bernard TJ, Fullerton HJ, Gordon A, deVeber G; International Pediatric Stroke Study Group . Antithrombotic treatments, outcomes, and prognostic factors in acute childhood-onset arterial ischaemic stroke: a multicentre, observational, cohort study. Lancet Neurol. 2009;8(12):1120-1127. doi:10.1016/S1474-4422(09)70241-8 - DOI - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. ; American Heart Association Stroke Council . 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46-e110. doi:10.1161/STR.0000000000000158 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
