

Early Palliative Care Consultation in the Medical ICU: A Cluster Randomized Crossover Trial
- PMID: 31609772
- PMCID: PMC6861688
- DOI: 10.1097/CCM.0000000000004016
Early Palliative Care Consultation in the Medical ICU: A Cluster Randomized Crossover Trial
Abstract
Objectives: To assess the impact of early triggered palliative care consultation on the outcomes of high-risk ICU patients.
Design: Single-center cluster randomized crossover trial.
Setting: Two medical ICUs at Barnes Jewish Hospital.
Patients: Patients (n = 199) admitted to the medical ICUs from August 2017 to May 2018 with a positive palliative care screen indicating high risk for morbidity or mortality.
Interventions: The medical ICUs were randomized to intervention or usual care followed by washout and crossover, with independent assignment of patients to each ICU at admission. Intervention arm patients received a palliative care consultation from an interprofessional team led by board-certified palliative care providers within 48 hours of ICU admission.
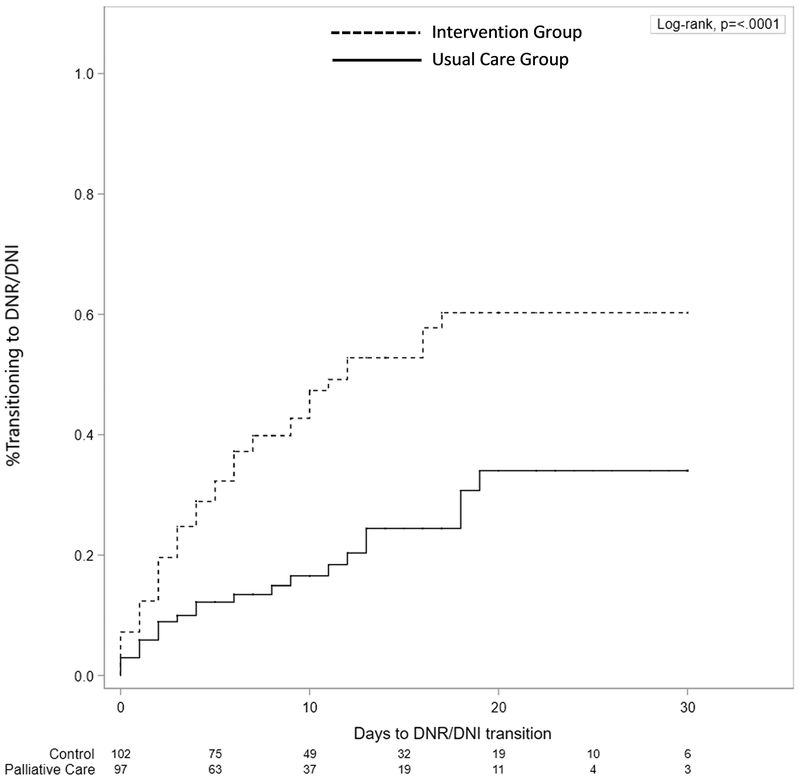
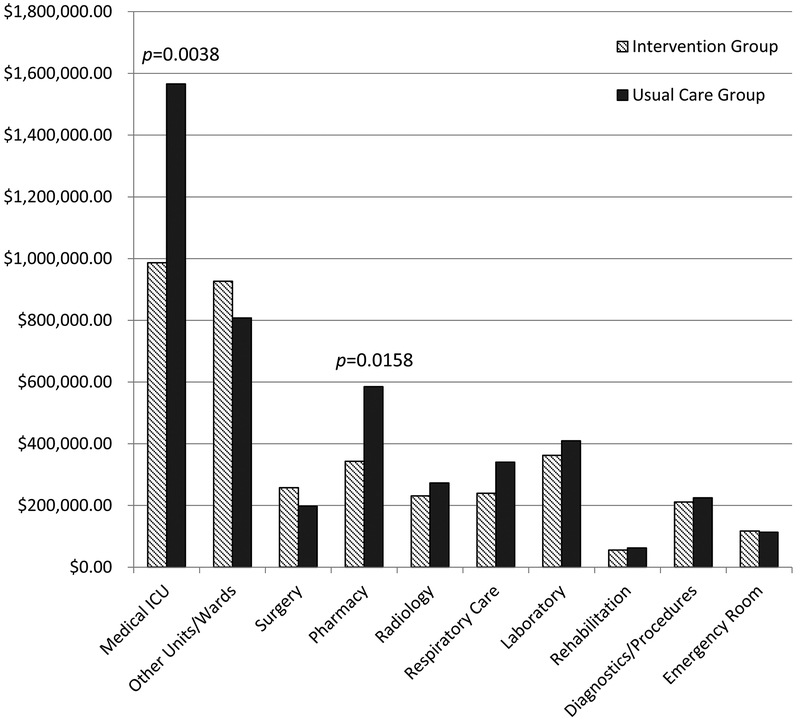
Measurements and main results: Ninety-seven patients (48.7%) were assigned to the intervention and 102 (51.3%) to usual care. Transition to do-not-resuscitate/do-not-intubate occurred earlier and significantly more often in the intervention group than the control group (50.5% vs 23.4%; p < 0.0001). The intervention group had significantly more transfers to hospice care (18.6% vs 4.9%; p < 0.01) with fewer ventilator days (median 4 vs 6 d; p < 0.05), tracheostomies performed (1% vs 7.8%; p < 0.05), and postdischarge emergency department visits and/or readmissions (17.3% vs 38.9%; p < 0.01). Although total operating cost was not significantly different, medical ICU (p < 0.01) and pharmacy (p < 0.05) operating costs were significantly lower in the intervention group. There was no significant difference in ICU length of stay (median 5 vs 5.5 d), hospital length of stay (median 10 vs 11 d), in-hospital mortality (22.6% vs 29.4%), or 30-day mortality between groups (35.1% vs 36.3%) (p > 0.05).
Conclusions: Early triggered palliative care consultation was associated with greater transition to do-not-resuscitate/do-not-intubate and to hospice care, as well as decreased ICU and post-ICU healthcare resource utilization. Our study suggests that routine palliative care consultation may positively impact the care of high risk, critically ill patients.
Trial registration: ClinicalTrials.gov NCT03263143.
Conflict of interest statement
Figures
Comment in
-
In high-risk ICU patients, early palliative care consultation increased transition to DNR/DNI status.Ann Intern Med. 2020 Mar 17;172(6):JC30. doi: 10.7326/ACPJ202003170-030. Ann Intern Med. 2020. PMID: 32176896 No abstract available.
-
High-Value Palliative Care in Critical Illness.Crit Care Med. 2020 Apr;48(4):e341. doi: 10.1097/CCM.0000000000004215. Crit Care Med. 2020. PMID: 32205636 No abstract available.
-
The authors reply.Crit Care Med. 2020 Apr;48(4):e342. doi: 10.1097/CCM.0000000000004264. Crit Care Med. 2020. PMID: 32205637 No abstract available.
References
-
- Devlin JW, Skrobik Y, Gélinas C, et al.: Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med 2018; 46:e825–e873. - PubMed
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al.: Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004; 32:638–643. - PubMed
-
- Truog RD, Campbell ML, Curtis JR, et al.: Recommendations for end-of-life care in the intensive care unit: a consensus statement by the American College [corrected] of Critical Care Medicine. Crit Care Med. 2008;36(3):953–963. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
