

Causes of Horner Syndrome: A Study of 318 Patients
- PMID: 31609831
- PMCID: PMC7148177
- DOI: 10.1097/WNO.0000000000000844
Causes of Horner Syndrome: A Study of 318 Patients
Abstract
Background: Some reports have indicated that when a cause for Horner syndrome can be determined, it is most often chest and neck tumors and stroke. Others have suggested that Horner syndrome is more frequently caused by surgical procedures in the neck and chest. These differences may be explained by disparate accrual methods. Therefore, we decided to compare the cause of Horner syndrome in cases where the diagnosis was confirmed by apraclonidine testing conducted by ophthalmologists to cases in which the diagnosis was made entirely on clinical grounds mostly by nonophthalmologists.
Methods: We applied a new search engine to the inpatient and outpatient electronic medical records text at the University of Michigan Medical Center from 1996 to 2018 for Horner syndrome with and without pharmacologic confirmation through ocular instillation of apraclonidine 0.5%. Among apraclonidine-confirmed cases, 159 met inclusion criteria. Among apraclonidine-unconfirmed cases, more than 2,000 cases were identified, so that we included only the first 159 cases that met inclusion criteria. In these 318 cases, we documented patient demographics, ophthalmologic features, imaging, underlying cause, and whether the cause was discovered before or after the diagnosis of Horner syndrome.
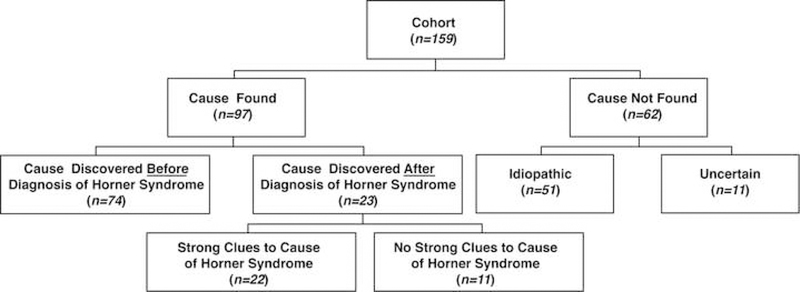
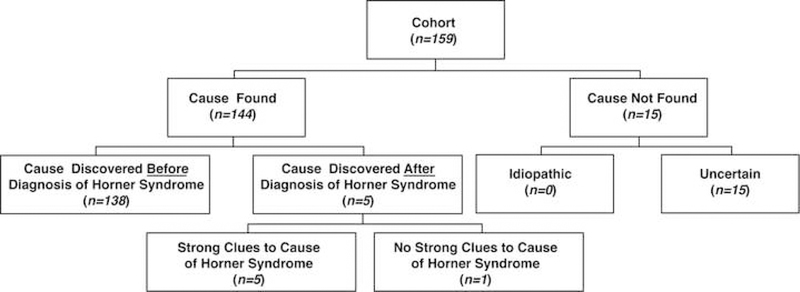
Results: In the cohort of 159 apraclonidine-confirmed cases of Horner syndrome, a cause was identified in 97 (61%). Procedures in the neck, chest, skull base, and paraspinal region accounted for most of the identified causes, with cervical carotid dissection the next most common cause. In a cohort of 159 cases of Horner syndrome not tested with apraclonidine because the clinical diagnosis appeared firm, procedures again accounted for the largest percentage, but tumor was the next most common cause. In both groups, when a cause for Horner syndrome could be identified, that cause was nearly always known before Horner syndrome was identified. However, in an important minority of cases, mostly involving carotid dissection or tumor, the identification of Horner syndrome was critical to the discovery of those conditions.
Conclusions: The prevalence of causes of Horner syndrome depends on the accrual method. Among pharmacologically-confirmed cases, the cause was often undetermined or due to a preceding neck or chest procedure. Among pharmacologically-unconfirmed cases, a substantial proportion had also been caused by neck and chest procedures, but tumors in that region were also common. When a cause of Horner syndrome was found in both cohorts, it was usually known before Horner syndrome was discovered, making Horner syndrome an afterthought. However, in an important minority of cases where the cause was not yet known, the identification of Horner syndrome was valuable in leading to important diagnoses such as carotid dissection and tumor.
Conflict of interest statement
There is no conflict of interest to disclose.
Figures
References
-
- Walton KA, Buono LM. Horner syndrome. Curr Opin Ophthalmol 2003;14:357–363 - PubMed
-
- Giles CL, Henderson JW. Horner’s syndrome: an analysis of 216 cases. Am J Ophthalmol 1958;46:289–296. - PubMed
-
- Keane JR. Oculosympathetic paresis. Analysis of 100 hospitalized patients. Arch Neurol 1979;36:13–15. - PubMed
-
- Maloney WF, Younge BR, Moyer NJ. Evaluation of the causes and accuracy of pharmacologic localization in Horner’s syndrome. Am J Ophthalmol 1980;90:394–402 - PubMed
-
- Almog Y, Gepstein R, Kesler A. Diagnostic value of imaging in Horner syndrome in adults. J Neuroophthalmol 2010;30:7–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
