

Hypoxia-inducible factor-1α is the therapeutic target of the SGLT2 inhibitor for diabetic nephropathy
- PMID: 31611596
- PMCID: PMC6791873
- DOI: 10.1038/s41598-019-51343-1
Hypoxia-inducible factor-1α is the therapeutic target of the SGLT2 inhibitor for diabetic nephropathy
Abstract
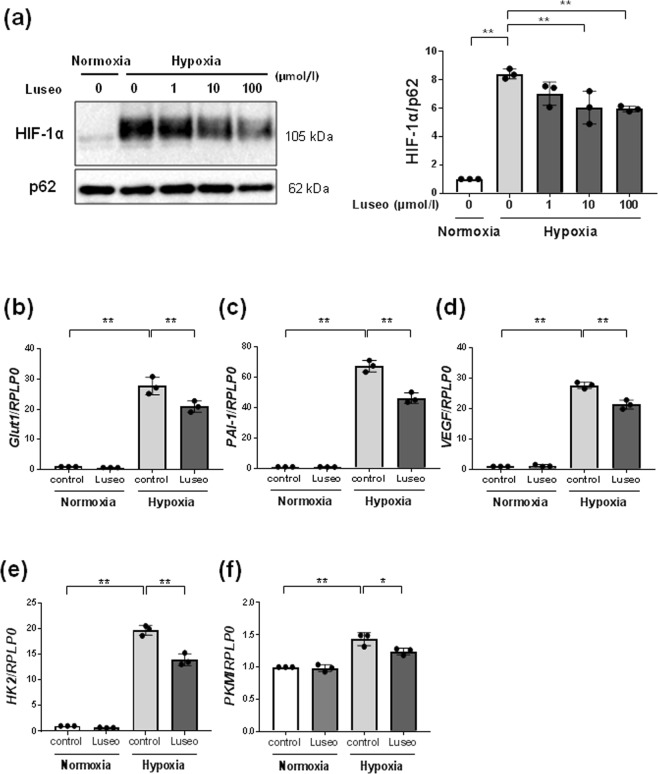
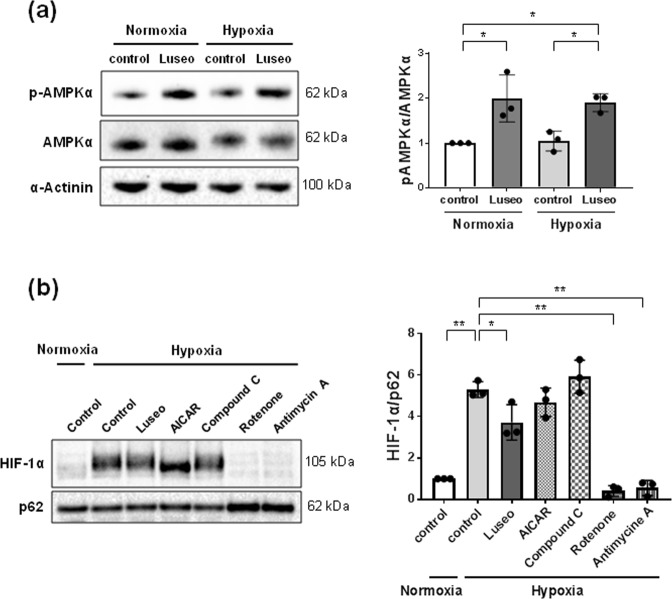
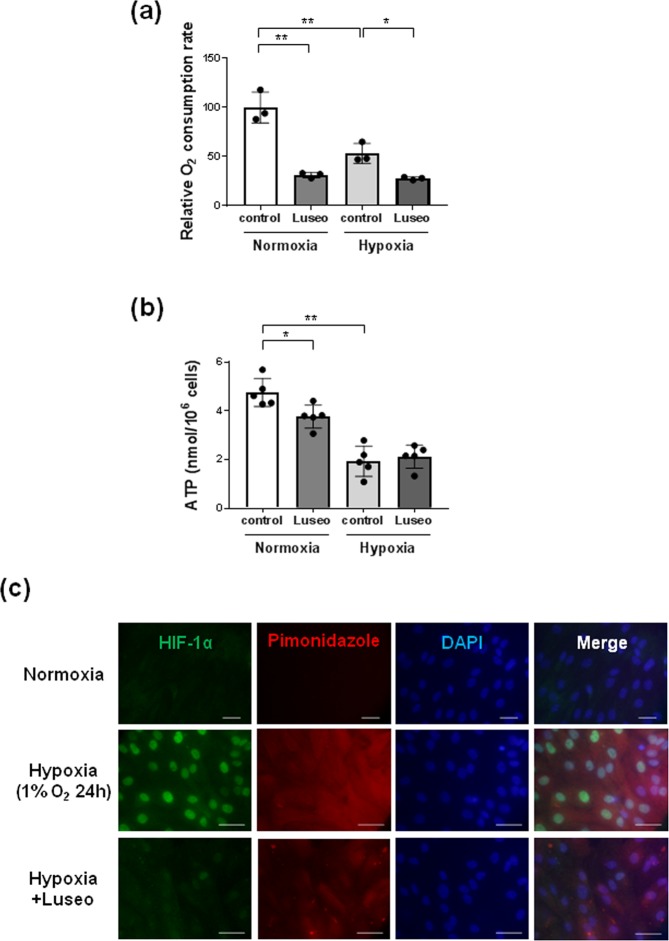
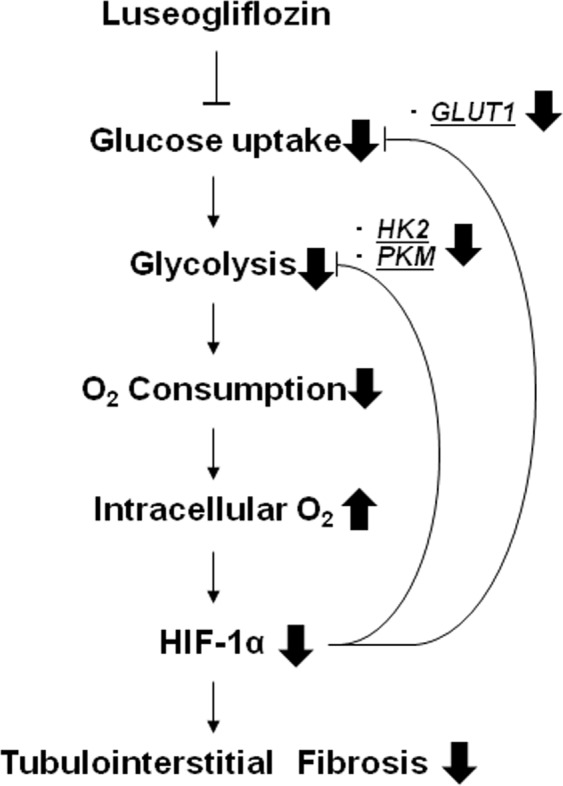
Previous studies have demonstrated intrarenal hypoxia in patients with diabetes. Hypoxia-inducible factor (HIF)-1 plays an important role in hypoxia-induced tubulointerstitial fibrosis. Recent clinical trials have confirmed the renoprotective action of SGLT2 inhibitors in diabetic nephropathy. We explored the effects of an SGLT2 inhibitor, luseogliflozin on HIF-1α expression in human renal proximal tubular epithelial cells (HRPTECs). Luseogliflozin significantly inhibited hypoxia-induced HIF-1α protein expression in HRPTECs. In addition, luseogliflozin inhibited hypoxia-induced the expression of the HIF-1α target genes PAI-1, VEGF, GLUT1, HK2 and PKM. Although luseogliflozin increased phosphorylated-AMP-activated protein kinase α (p-AMPKα) levels, the AMPK activator AICAR did not changed hypoxia-induced HIF-1α expression. Luseogliflozin suppressed the oxygen consumption rate in HRPTECs, and subsequently decreased hypoxia-sensitive dye, pimonidazole staining under hypoxia, suggesting that luseogliflozin promoted the degradation of HIF-1α protein by redistribution of intracellular oxygen. To confirm the inhibitory effect of luseogliflozin on hypoxia-induced HIF-1α protein in vivo, we treated male diabetic db/db mice with luseogliflozin for 8 to 16 weeks. Luseogliflozin attenuated cortical tubular HIF-1α expression, tubular injury and interstitial fibronectin in db/db mice. Together, luseogliflozin inhibits hypoxia-induced HIF-1α accumulation by suppressing mitochondrial oxygen consumption. The SGLT2 inhibitors may protect diabetic kidneys by therapeutically targeting HIF-1α protein.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
