

The relative importance of factors predicting outcome for myeloma patients at different ages: results from 3894 patients in the Myeloma XI trial
- PMID: 31611625
- PMCID: PMC7214257
- DOI: 10.1038/s41375-019-0595-5
The relative importance of factors predicting outcome for myeloma patients at different ages: results from 3894 patients in the Myeloma XI trial
Abstract
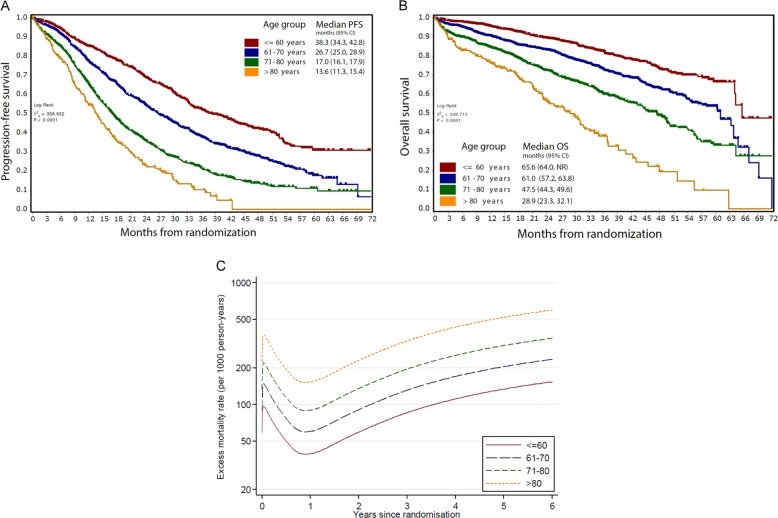
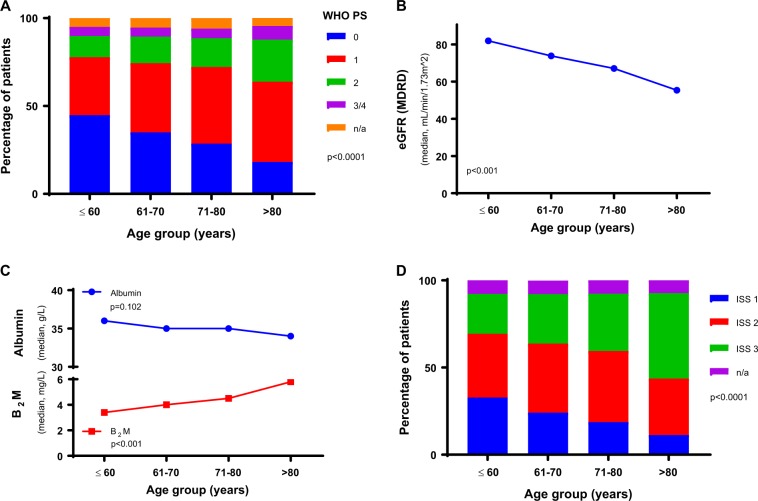
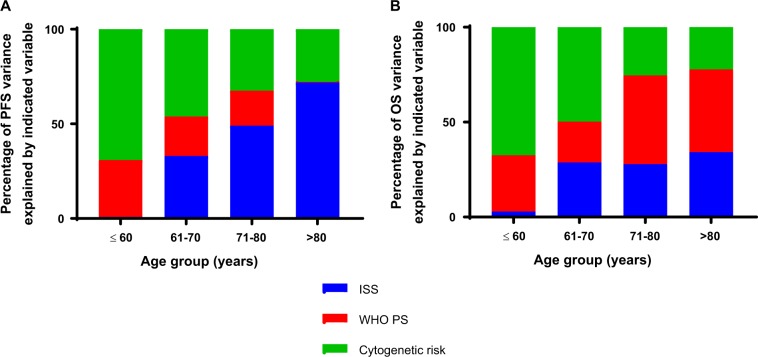
Disease factors such as tumor burden and molecular risk affect myeloma patient outcomes as well as patient factors that impact the capacity to deliver treatment. How the relative importance of these factors changes with patient age has not previously been investigated comprehensively. We analyzed data from 3894 patients of all ages uniformly treated in a large clinical trial of myeloma patients, Myeloma XI. Even with novel therapeutic approaches progression-free survival (PFS) and overall survival (OS) are affected by age with a stepwise reduction in PFS and OS with each decade increase. Renal function deteriorated with increasing age whilst the frequency of t(4;14) and del(17p) decreased and gain(1q) increased. The relative contribution of performance status, international staging score and molecular risk to progression-free and overall survival varied by age group. Molecular events have a larger effect on outcome in younger patients with their relative contribution diminishing in the elderly. Performance status is important for patient outcome at all ages suggesting that physical frailty may be a more important predictor of outcome than age itself. Significant differences in the factors driving patient outcomes at different ages are important to consider as we design disease segmentation strategies to deliver personalized treatment approaches.
Conflict of interest statement
CP
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
