

Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane Versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA)
- PMID: 31612359
- PMCID: PMC6822789
- DOI: 10.1007/s12325-019-01055-9
Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane Versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA)
Abstract
Introduction: Inhaled low-dose methoxyflurane is approved in Europe for emergency relief of moderate-to-severe trauma-related pain in adults, but data versus active comparators are sparse. The phase IIIb Methoxyflurane in Emergency Department in ITAly (MEDITA) trial investigated the analgesic efficacy, practicality and safety of methoxyflurane versus standard analgesic treatment (SAT) for acute trauma pain.
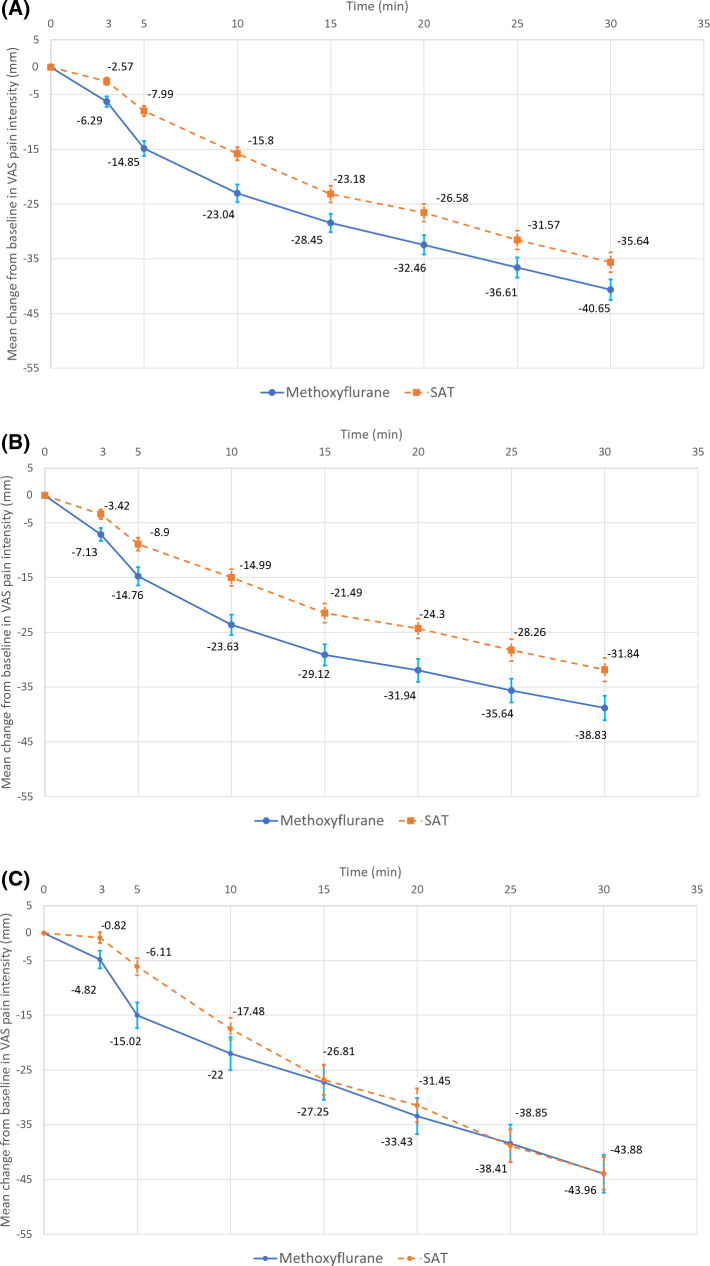
Methods: This was a randomised, active-controlled, parallel-group, open-label trial conducted in 15 Italian emergency units. Adults with limb trauma and pain score ≥ 4 on numerical rating scale (NRS) were randomised 1:1 to inhaled methoxyflurane 3 mL or SAT [intravenously administered (IV) morphine 0.1 mg/kg for severe pain (NRS ≥ 7); IV paracetamol 1 g or IV ketoprofen 100 mg for moderate pain (NRS 4-6)]. The primary endpoint was overall change in visual analogue scale (VAS) pain intensity from baseline (time of randomisation) to 3, 5 and 10 min. Non-inferiority and superiority of methoxyflurane versus SAT were concluded if the upper 95% confidence interval (CI) for the treatment comparison (methoxyflurane-SAT) was less than 1 and less than 0, respectively.
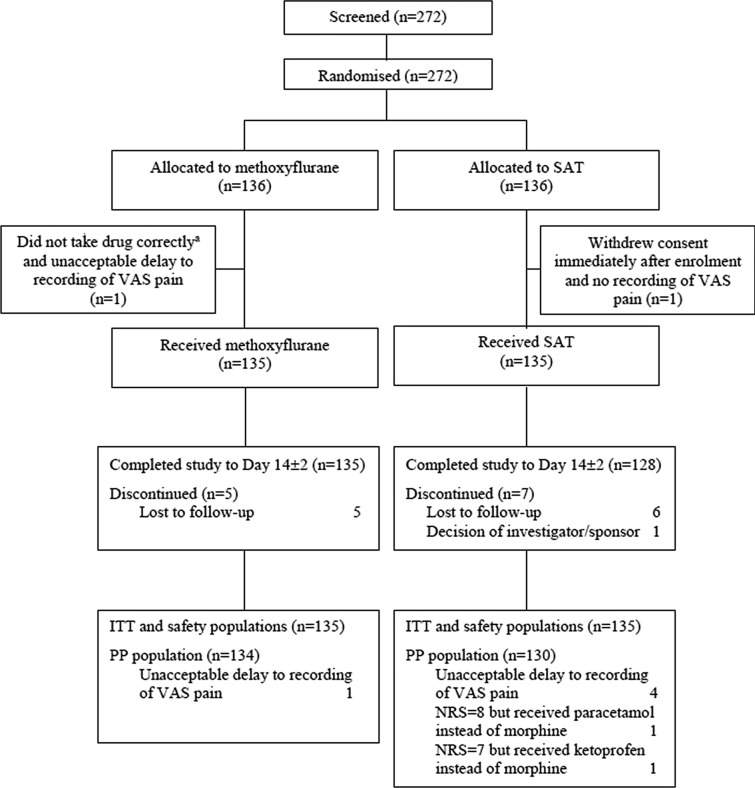
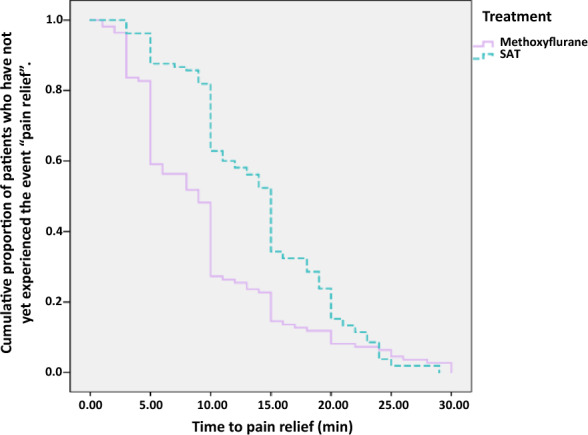
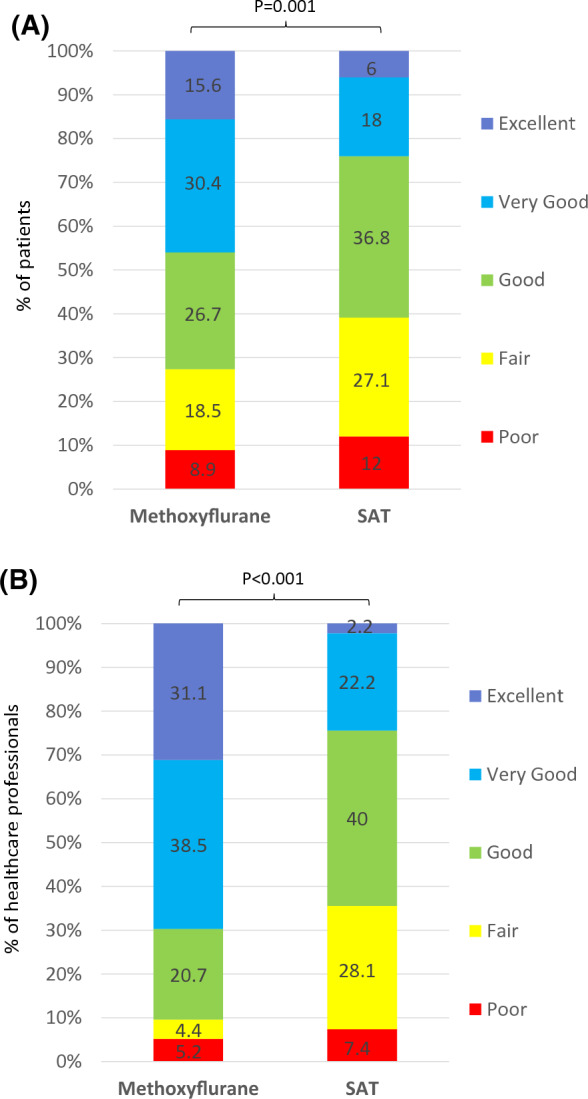
Results: Between 8 February 2018 and 8 February 2019, 272 patients were randomised (136 per treatment group). A total of 270 patients (mean age 51 years; 49% male; 34% with severe pain; mean baseline VAS 67 mm) were treated and analysed for efficacy and safety. Superiority of methoxyflurane was demonstrated for moderate-to-severe pain (adjusted mean treatment difference - 5.94 mm; 95% CI - 8.83, - 3.06 mm), moderate pain (- 5.97 mm; 95% CI - 9.55, - 2.39 mm) and severe pain (- 5.54 mm; 95% CI - 10.49, - 0.59 mm). Median onset of pain relief was 9 min for methoxyflurane and 15 min for SAT. Practicality of methoxyflurane treatment was rated "Excellent", "Very Good" or "Good" by 90% of clinicians vs. 64% for SAT. Adverse events (all non-serious) were reported by 17% of methoxyflurane-treated patients and 3% of SAT-treated patients.
Conclusion: Methoxyflurane provided superior pain relief to SAT in patients with moderate-to-severe trauma pain and may offer a simple, fast, effective non-opioid treatment option.
Trial registration: Trial registered with EudraCT (2017-001565-25) on 2 March 2018 and ClinicalTrials.gov (NCT03585374) on 13 July 2018.
Funding: Mundipharma Pharmaceuticals S.r.l.
Keywords: Acute pain; Analgesic; Emergency department; Methoxyflurane; Morphine; Non-steroidal anti-inflammatory drug; Paracetamol; Penthrox; Prehospital; Trauma.
Conflict of interest statement
Elisabetta Bonafede is an employee of the clinical research organisation that conducted the study. Antonella Sblendido is an employee of Mundipharma Pharmaceuticals S.r.l. Amedeo Soldi is an employee of Mundipharma Pharmaceuticals S.r.l. Alberto Farina is an employee of Mundipharma Pharmaceuticals S.r.l. Sebastiano Mercadante, Antonio Voza, Sossio Serra, Germana Ruggiano, Andrea Fabbri, Giuseppe Carpinteri, Gianfilippo Gangitano and Fabio Intelligente have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
