

Impact of Clinical Specialty Setting and Geographic Regions on Disease Management in Patients with Psoriatic Arthritis in the United States: A Multicenter Observational Study
- PMID: 31612380
- PMCID: PMC6872709
- DOI: 10.1007/s40257-019-00470-6
Impact of Clinical Specialty Setting and Geographic Regions on Disease Management in Patients with Psoriatic Arthritis in the United States: A Multicenter Observational Study
Abstract
Background: Information on the factors that influence treatment management decisions for psoriatic arthritis (PsA) is limited.
Objective: Our objective was to evaluate the impact of clinical specialty setting and geographic region on the management of patients with PsA in the USA.
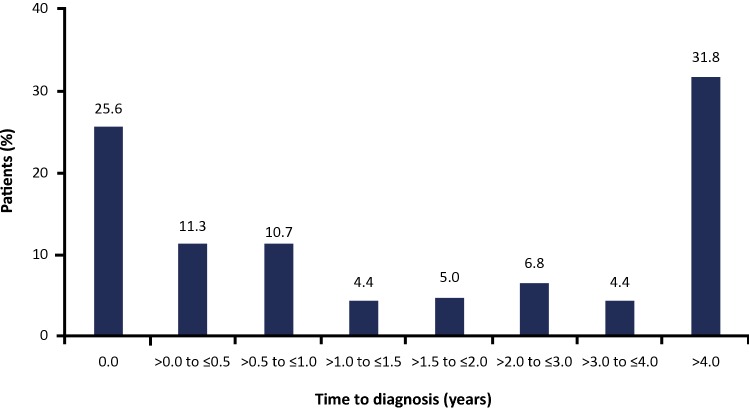
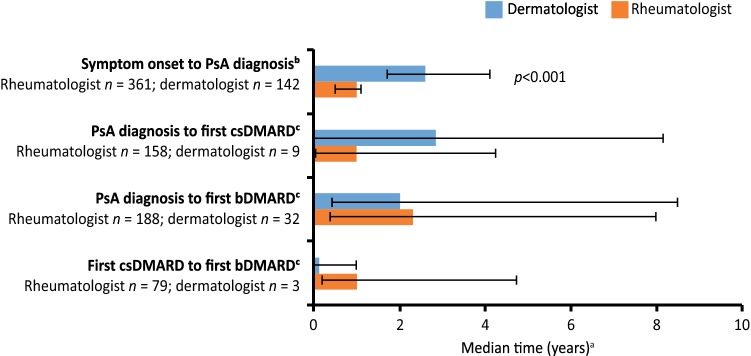
Methods: LOOP was a multicenter, cross-sectional, observational study conducted across 44 sites in the USA. Patients were aged ≥ 18 years with a suspected or established diagnosis of PsA and were routinely visiting a rheumatologist or dermatologist. All patients enrolled in the study were assessed by both a rheumatologist and a dermatologist. Primary outcomes were the times from symptom onset to PsA diagnosis; PsA diagnosis to first conventional synthetic disease-modifying antirheumatic drug (csDMARD); PsA diagnosis to first biologic DMARD (bDMARD); and first csDMARD to first bDMARD.
Results: Of 681 patients enrolled in the study, 513 had a confirmed diagnosis of PsA and were included in this analysis. More patients were recruited by rheumatologists (71.3%) than by dermatologists (28.7%). The median time from symptom onset to diagnosis of PsA was significantly shorter for patients enrolled by rheumatologists than for those enrolled by dermatologists (1.0 vs. 2.6 years; p < 0.001). Disease activity and burden were generally similar across enrolling specialties. However, patients in western areas of the USA had less severe disease than those in central or eastern areas, including measures of joint involvement, enthesitis, and dactylitis.
Conclusions: There was a substantial delay in the time from symptom onset to diagnosis in this study population, and this was significantly longer for patients enrolled in the dermatology versus the rheumatology setting. This supports the need for collaboration across specialties to ensure faster recognition and treatment of PsA.
Conflict of interest statement
P.J. Mease has received research grants, consulting fees, and/or speaker’s fees from AbbVie, Amgen, Bristol-Myers Squib, Celgene, Galapagos, Genentech, Gilead, Janssen, Lilly, Novartis, Pfizer, Sun Pharma, and UCB. B. Lockshin has received research grants, consulting fees, and speaker’s fees from AbbVie, Janssen, Lilly, and Novartis; has received research grants from Celgene and Strata; and is on the board of directors for the National Psoriasis Foundation. C. Liu has served as a speaker, on an advisory board, and/or as an investigator for AbbVie, Celgene, Janssen, Lilly, Novartis, Ortho, Regeneron, and Sanofi. E. Siegel has received research grants and acted as a speaker for and/or received consulting fees from AbbVie, Amgen, Celgene, Janssen, Lilly, Sanofi, and UCB. H. Richmond has received a research grant from AbbVie. M. Wu, L. Chen, and K. Douglas are employees of AbbVie and may own stock/options.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
