

Effect of a Nutritional and Behavioral Intervention on Energy-Reduced Mediterranean Diet Adherence Among Patients With Metabolic Syndrome: Interim Analysis of the PREDIMED-Plus Randomized Clinical Trial
- PMID: 31613346
- PMCID: PMC6802271
- DOI: 10.1001/jama.2019.14630
Effect of a Nutritional and Behavioral Intervention on Energy-Reduced Mediterranean Diet Adherence Among Patients With Metabolic Syndrome: Interim Analysis of the PREDIMED-Plus Randomized Clinical Trial
Abstract
Importance: High-quality dietary patterns may help prevent chronic disease, but limited data exist from randomized trials about the effects of nutritional and behavioral interventions on dietary changes.
Objective: To assess the effect of a nutritional and physical activity education program on dietary quality.
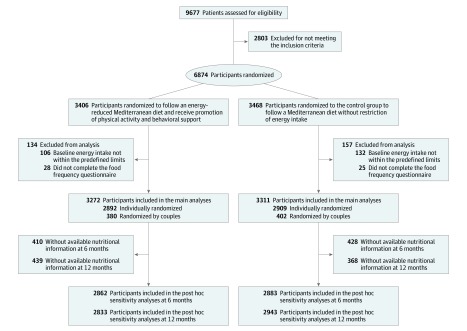
Design, setting, and participants: Preliminary exploratory interim analysis of an ongoing randomized trial. In 23 research centers in Spain, 6874 men and women aged 55 to 75 years with metabolic syndrome and no cardiovascular disease were enrolled in the trial between September 2013 and December 2016, with final data collection in March 2019.
Interventions: Participants were randomized to an intervention group that encouraged an energy-reduced Mediterranean diet, promoted physical activity, and provided behavioral support (n = 3406) or to a control group that encouraged an energy-unrestricted Mediterranean diet (n = 3468). All participants received allotments of extra-virgin olive oil (1 L/mo) and nuts (125 g/mo) for free.
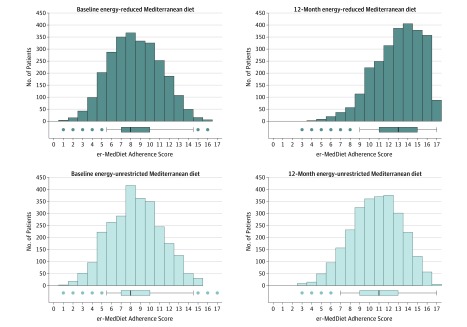
Main outcomes and measures: The primary outcome was 12-month change in adherence based on the energy-reduced Mediterranean diet (er-MedDiet) score (range, 0-17; higher scores indicate greater adherence; minimal clinically important difference, 1 point).
Results: Among 6874 randomized participants (mean [SD] age, 65.0 [4.9] years; 3406 [52%] men), 6583 (96%) completed the 12-month follow-up and were included in the main analysis. The mean (SD) er-MedDiet score was 8.5 (2.6) at baseline and 13.2 (2.7) at 12 months in the intervention group (increase, 4.7 [95% CI, 4.6-4.8]) and 8.6 (2.7) at baseline and 11.1 (2.8) at 12 months in the control group (increase, 2.5 [95% CI, 2.3-2.6]) (between-group difference, 2.2 [95% CI, 2.1-2.4]; P < .001).
Conclusions and relevance: In this preliminary analysis of an ongoing trial, an intervention that encouraged an energy-reduced Mediterranean diet and physical activity, compared with advice to follow an energy-unrestricted Mediterranean diet, resulted in a significantly greater increase in diet adherence after 12 months. Further evaluation of long-term cardiovascular effects is needed.
Trial registration: isrctn.com Identifier: ISRCTN89898870.
Conflict of interest statement
Figures
Comment in
-
Dietary Adherence in a Clinical Trial of a Nutritional and Behavioral Intervention.JAMA. 2019 Oct 15;322(15):1500. doi: 10.1001/jama.2019.15855. JAMA. 2019. PMID: 31613331 No abstract available.
References
-
- Abarca-Gomez L, Abdeen Z, Hamid Z, et al. ; NCD Risk Factor Collaboration (NCD-RisC) . Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627-2642. doi:10.1016/S0140-6736(17)32129-3 - DOI - PMC - PubMed
