

Implementing a structured model for osteoarthritis care in primary healthcare: A stepped-wedge cluster-randomised trial
- PMID: 31613885
- PMCID: PMC6793845
- DOI: 10.1371/journal.pmed.1002949
Implementing a structured model for osteoarthritis care in primary healthcare: A stepped-wedge cluster-randomised trial
Erratum in
-
Correction: Implementing a structured model for osteoarthritis care in primary healthcare: A stepped-wedge cluster-randomised trial.PLoS Med. 2019 Dec 19;16(12):e1002993. doi: 10.1371/journal.pmed.1002993. eCollection 2019 Dec. PLoS Med. 2019. PMID: 31856163 Free PMC article.
Abstract
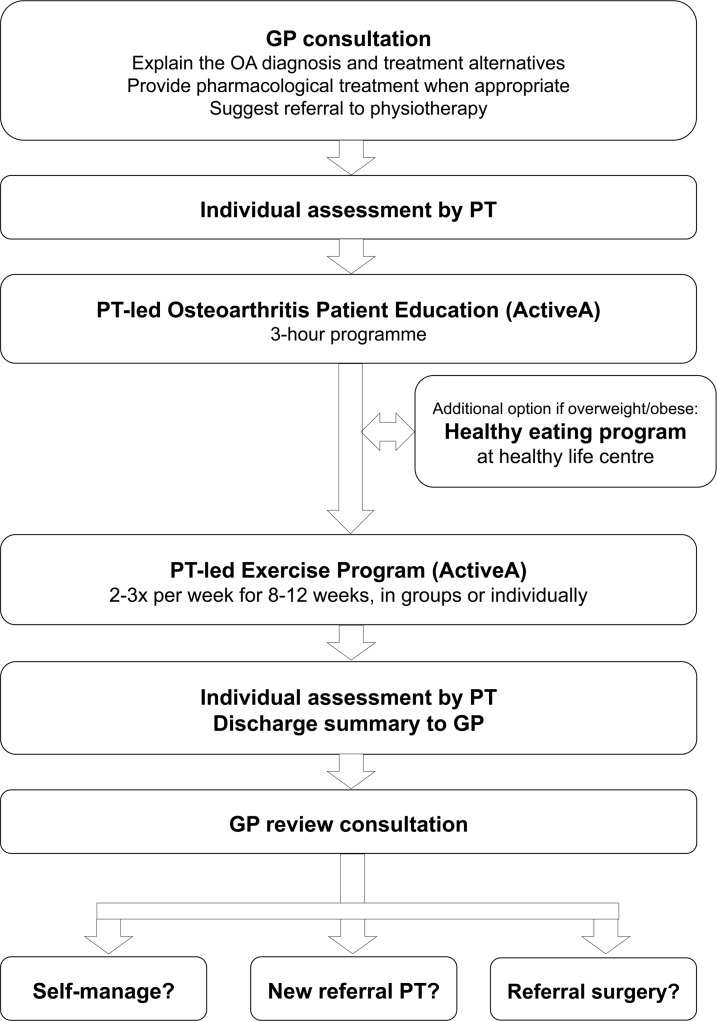
Background: To improve quality of care for patients with hip and knee osteoarthritis (OA), a structured model for integrated OA care was developed based on international recommendations. The objective of this study was to assess the effectiveness of this model in primary care.
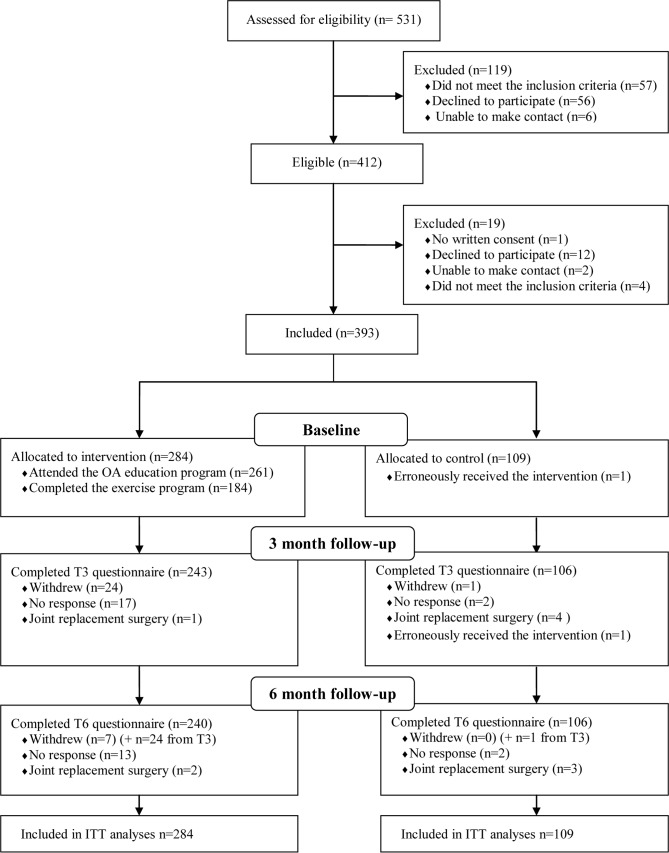
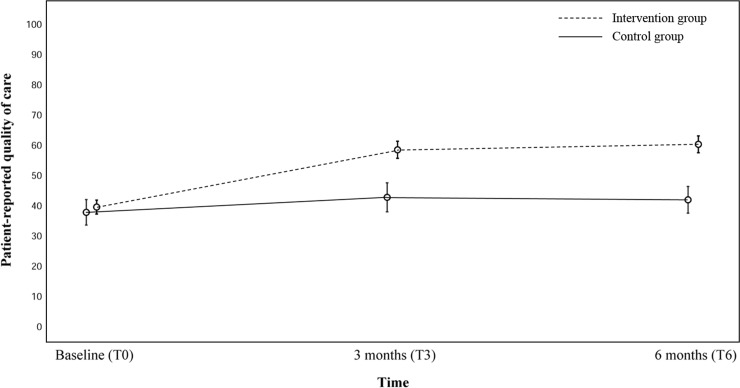
Methods and findings: We conducted a cluster-randomised controlled trial with stepped-wedge cohort design in 6 Norwegian municipalities (clusters) between January 2015 and October 2017. The randomised order was concealed to the clusters until the time of crossover from the control to the intervention phase. The intervention was implementation of the SAMBA model, facilitated by interactive workshops for general practitioners and physiotherapists with an update on OA treatment recommendations. Patients in the intervention group attended a physiotherapist-led OA education and individually tailored exercise programme for 8-12 weeks. The primary outcome was patient-reported quality of care (OsteoArthritis Quality Indicator questionnaire; 0-100, 100 = optimal quality) at 6 months. Secondary outcomes included patient-reported referrals to physiotherapy, magnetic resonance imaging (MRI), and orthopaedic surgeon consultation; patients' satisfaction with care; physical activity level; and proportion of patients who were overweight or obese (body mass index ≥ 25 kg/m2). In all, 40 of 80 general practitioners (mean age [SD] 50 [12] years, 42% females) and 37 of 64 physiotherapists (mean age [SD] 42 [8] years, 65% females) participated. They identified 531 patients, of which 393 patients (mean age [SD] 64 [10] years, 71% females) with symptomatic hip or knee OA were included. Among these, 109 patients were recruited during the control periods (control group), and 284 patients were recruited during interventions periods (intervention group). The patients in the intervention group reported significantly higher quality of care (score of 60 versus 41, mean difference 18.9; 95% CI 12.7, 25.1; p < 0.001) and higher satisfaction with OA care (odds ratio [OR] 12.1; 95% CI 6.44, 22.72; p < 0.001) compared to patients in the control group. The increase in quality of care was close to, but below, the pre-specified minimal important change. In the intervention group, a higher proportion was referred to physiotherapy (OR 2.5; 95% CI 1.08, 5.73; p = 0.03), a higher proportion fulfilled physical activity recommendations (OR 9.3; 95% CI 2.87, 30.37; p < 0.001), and a lower proportion was referred to an orthopaedic surgeon (OR 0.3; 95% CI 0.08, 0.80; p = 0.02), as compared to the control group. There were no significant group differences regarding referral to MRI (OR 0.6; 95% CI 0.13, 2.38; p = 0.42) and proportion of patients who were overweight or obese (OR 1.3; 95% CI 0.70, 2.51; p = 0.34). Study limitations include the imbalance in patient group size, which may have been due to an increased attention to OA patients among the health professionals during the intervention phase, and a potential recruitment bias as the patient participants were identified by their health professionals.
Conclusions: In this study, a structured model in primary care resulted in higher quality of OA care as compared to usual care. Future studies should explore ways to implement the structured model for integrated OA care on a larger scale.
Trial registration: ClinicalTrials.gov NCT02333656.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- National Institute for Health and Care Excellence. Osteoarthritis: care and management in adults Clinical guideline (CG177). London: National Institute for Health and Care Excellence; 2014.
-
- Bitton R. The economic burden of osteoarthritis. Am J Manag Care. 2009;15:S230–5. - PubMed
-
- Ackerman IN, Pratt C, Gorelik A, Liew D. Projected burden of osteoarthritis and rheumatoid arthritis in Australia: a population-level analysis. Arthritis Care Res (Hoboken). 2018;70:877–83. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
