

The trial to reduce antimicrobial use in nursing home residents with Alzheimer's disease and other dementias: study protocol for a cluster randomized controlled trial
- PMID: 31615540
- PMCID: PMC6794759
- DOI: 10.1186/s13063-019-3675-y
The trial to reduce antimicrobial use in nursing home residents with Alzheimer's disease and other dementias: study protocol for a cluster randomized controlled trial
Abstract
Background: Infections are common in nursing home (NH) residents with advanced dementia but are often managed inappropriately. Antimicrobials are extensively prescribed, but frequently with insufficient evidence to support a bacterial infection, promoting the emergence of multidrug-resistant organisms. Moreover, the benefits of antimicrobials remain unclear in these seriously ill residents for whom comfort is often the goal of care. Prior NH infection management interventions evaluated in randomized clinical trials (RCTs) did not consider patient preferences and lack evidence to support their effectiveness in 'real-world' practice.
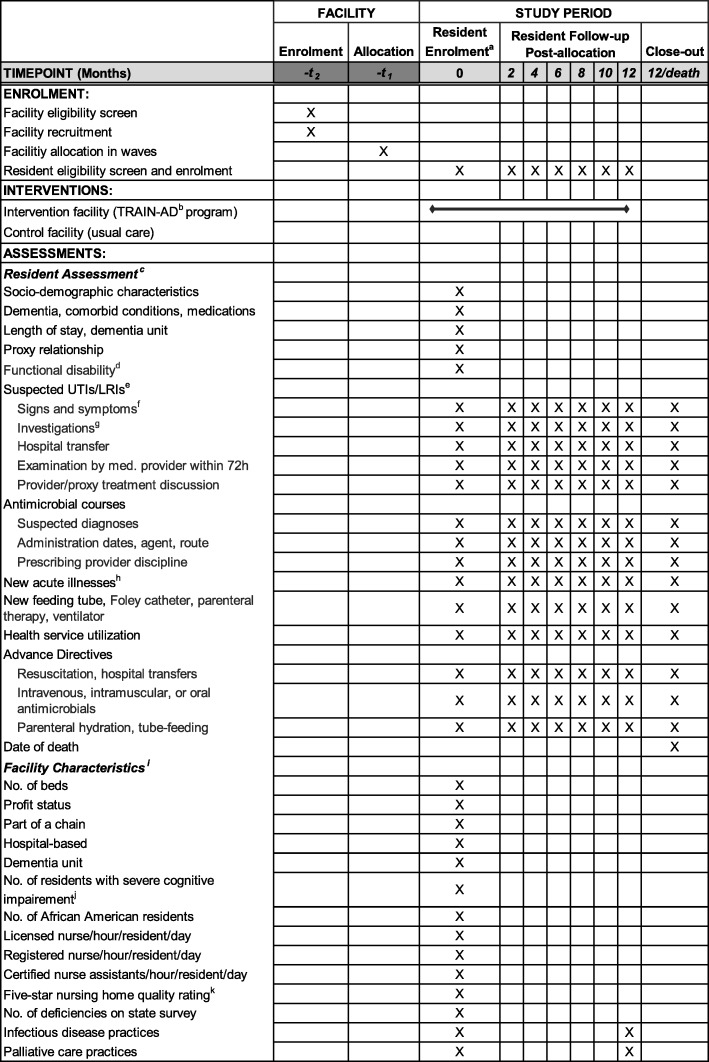
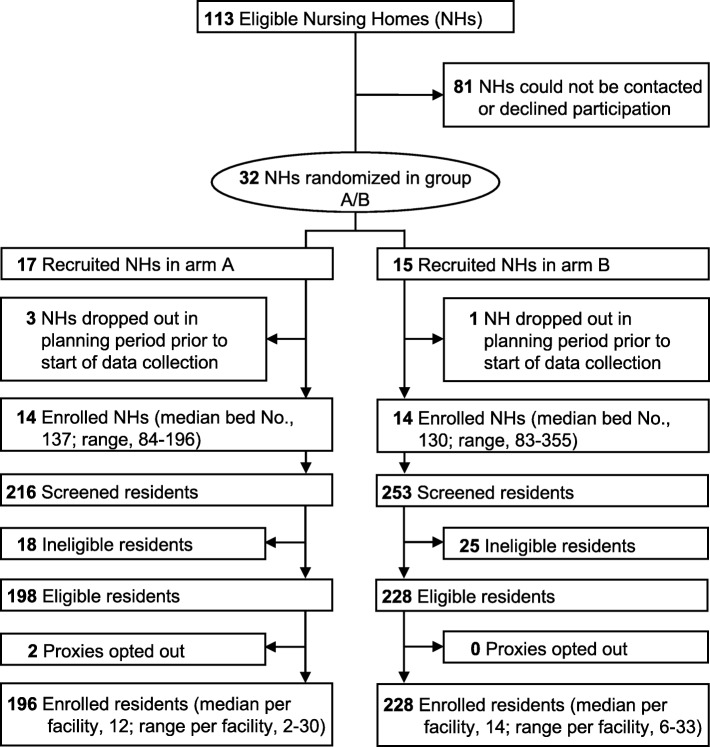
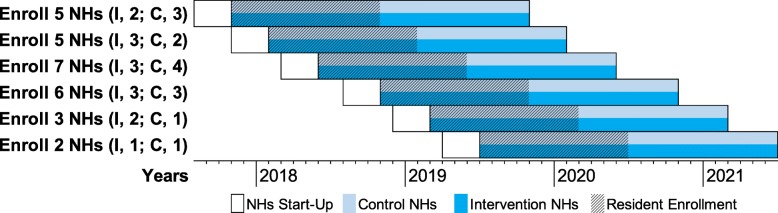
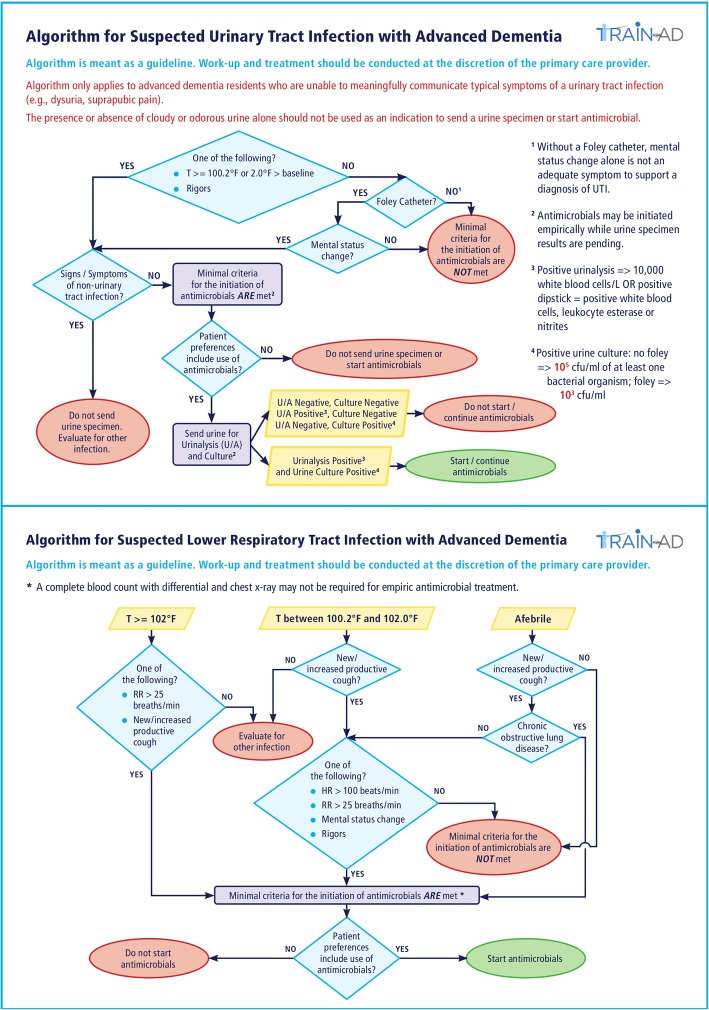
Methods: This report presents the rationale and methodology of TRAIN-AD (Trial to reduce antimicrobial use in nursing home residents with Alzheimer's disease and other dementias), a parallel group, cluster RCT evaluating a multicomponent intervention to improve infection management for suspected urinary tract infections (UTIs) and lower respiratory tract infections (LRIs) among NH residents with advanced dementia. TRAIN-AD is being conducted in 28 facilities in the Boston, USA, area randomized in waves using minimization to achieve a balance on key characteristics (N = 14 facilities/arm). The involvement of the facilities includes a 3-month start-up period and a 24-month implementation/data collection phase. Residents are enrolled during the first 12 months of the 24-month implementation period and followed for up to 12 months. Individual consent is waived, thus almost all eligible residents are enrolled (target sample size, N = 410). The intervention integrates infectious disease and palliative care principles and includes provider training delivered through multiple modalities (in-person seminar, online course, management algorithms, and prescribing feedback) and an information booklet for families. Control facilities employ usual care. The primary outcome, abstracted from the residents' charts, is the number of antimicrobial courses prescribed for UTIs and LRIs per person-year alive.
Discussion: TRAIN-AD is the first cluster RCT testing a multicomponent intervention to improve infection management in NH residents with advanced dementia. Its findings will provide an evidence base to support the benefit of a program addressing the critical clinical and public health problem of antimicrobial misuse in these seriously ill residents. Moreover, its hybrid efficacy-effectiveness design will inform the future conduct of cluster RCTs evaluating nonpharmacological interventions in the complex NH setting in a way that is both internally valid and adaptable to the 'real-world'.
Trial registration: ClinicalTrials.gov, NCT03244917 . Registered on 10 August 2017.
Keywords: Antimicrobials; Cluster randomized trial; Decision-making; Dementia; Goals of care; Implementation; Infections; Nursing homes; Palliative care; Pragmatic trial.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Alzheimer's Association. 2018 Alzheimer's disease facts and figures. https://www.alz.org/media/HomeOffice/Facts%20and%20Figures/facts-and-fig.... Accessed January 30, 2019.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
