

Potent Cell-Cycle Inhibition and Upregulation of Immune Response with Abemaciclib and Anastrozole in neoMONARCH, Phase II Neoadjuvant Study in HR+/HER2- Breast Cancer
- PMID: 31615937
- PMCID: PMC7498177
- DOI: 10.1158/1078-0432.CCR-19-1425
Potent Cell-Cycle Inhibition and Upregulation of Immune Response with Abemaciclib and Anastrozole in neoMONARCH, Phase II Neoadjuvant Study in HR+/HER2- Breast Cancer
Abstract
Purpose: neoMONARCH assessed the biological effects of abemaciclib in combination with anastrozole in the neoadjuvant setting.
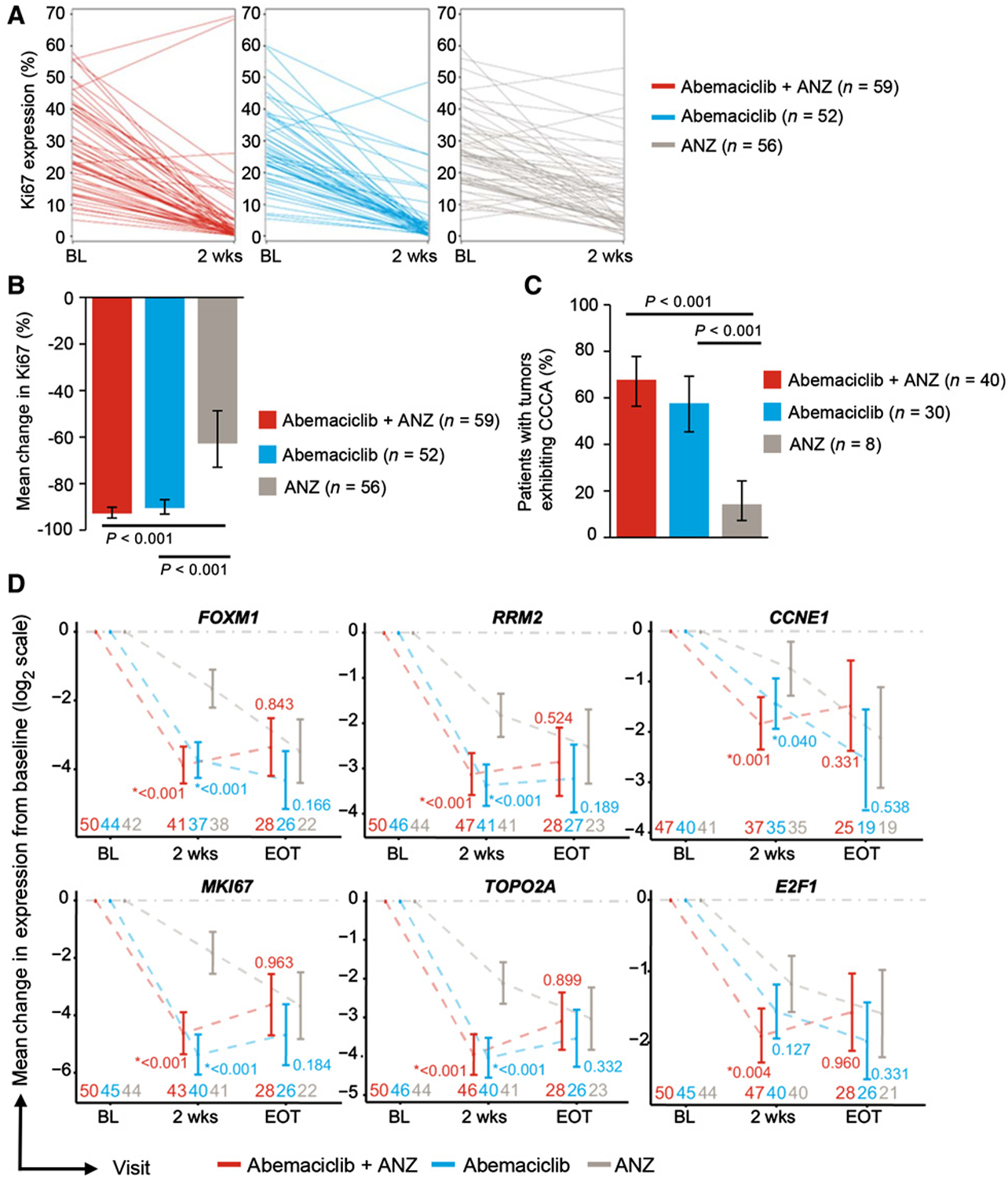
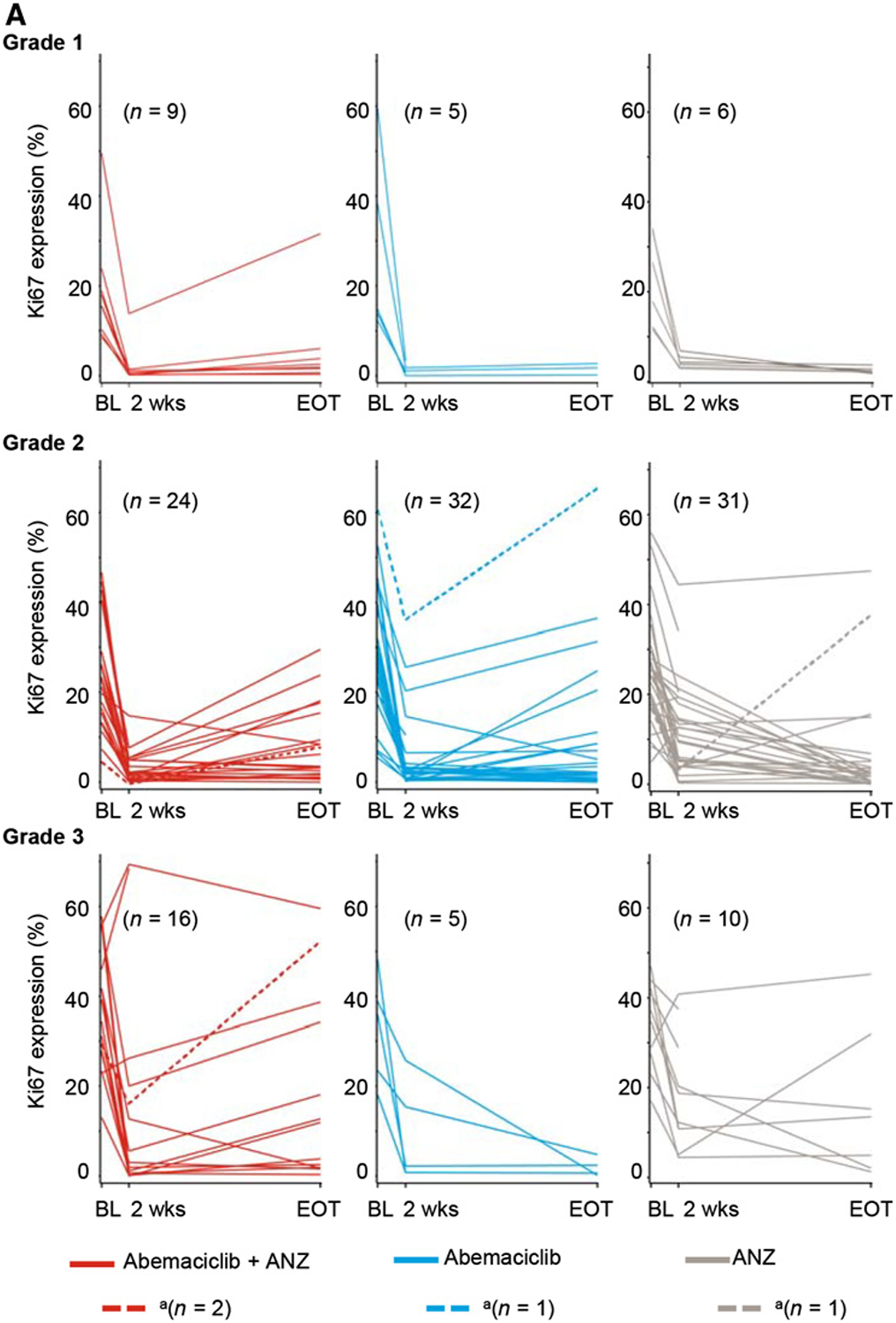
Patients and methods: Postmenopausal women with stage I-IIIB HR+/HER2- breast cancer were randomized to a 2-week lead-in of abemaciclib, anastrozole, or abemaciclib plus anastrozole followed by 14 weeks of the combination. The primary objective evaluated change in Ki67 from baseline to 2 weeks of treatment. Additional objectives included clinical, radiologic, and pathologic responses, safety, as well as gene expression changes related to cell proliferation and immune response.
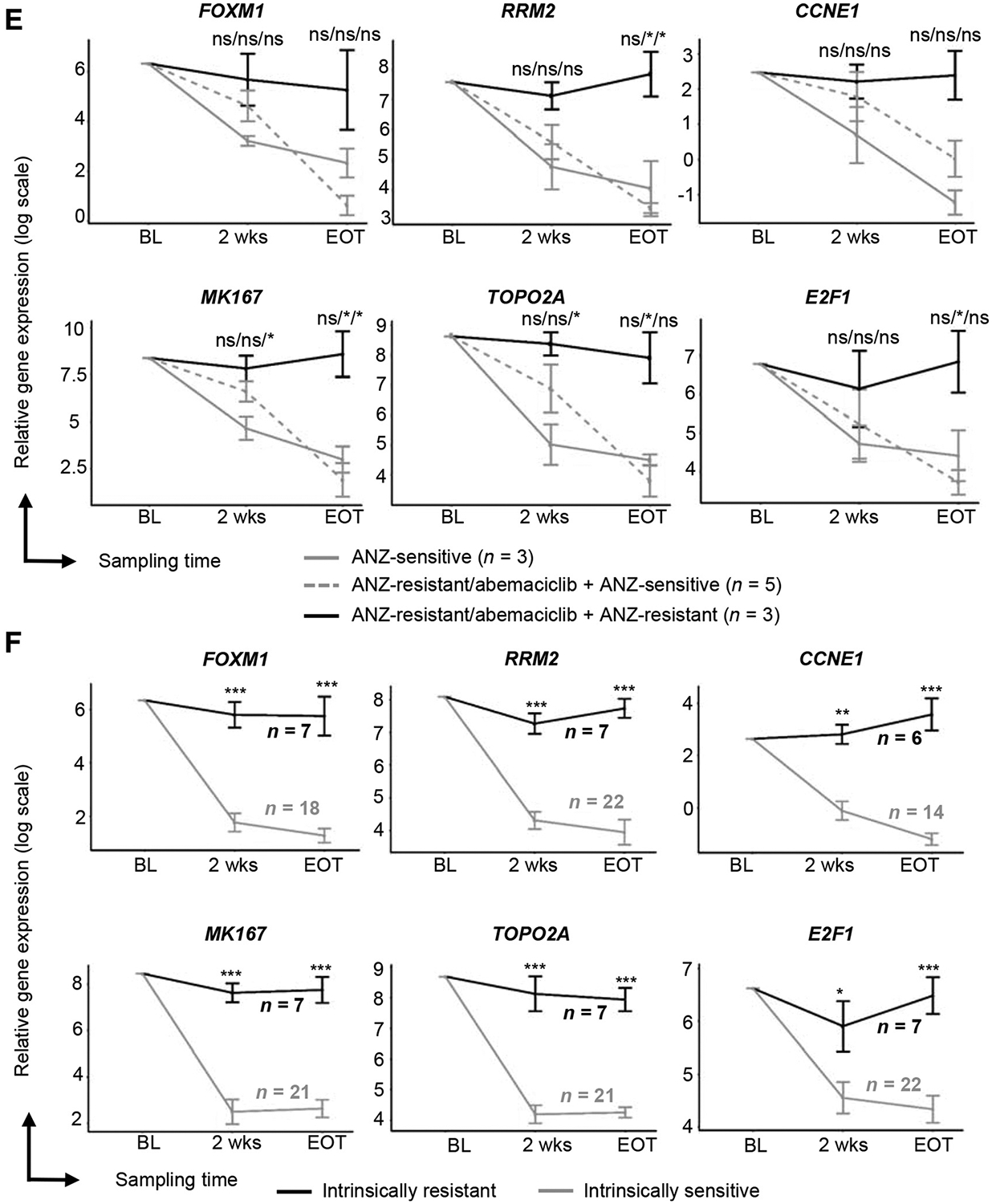
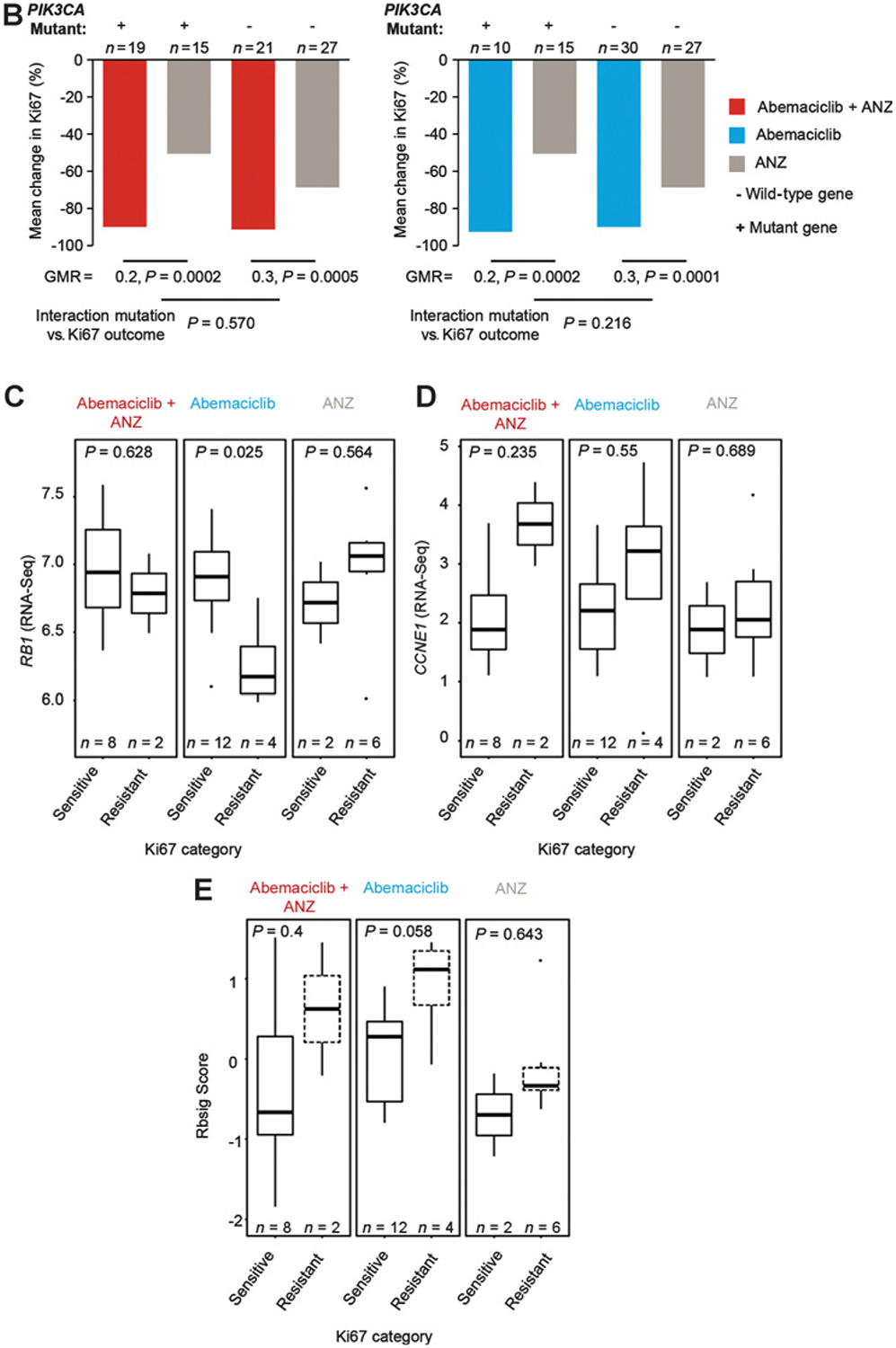
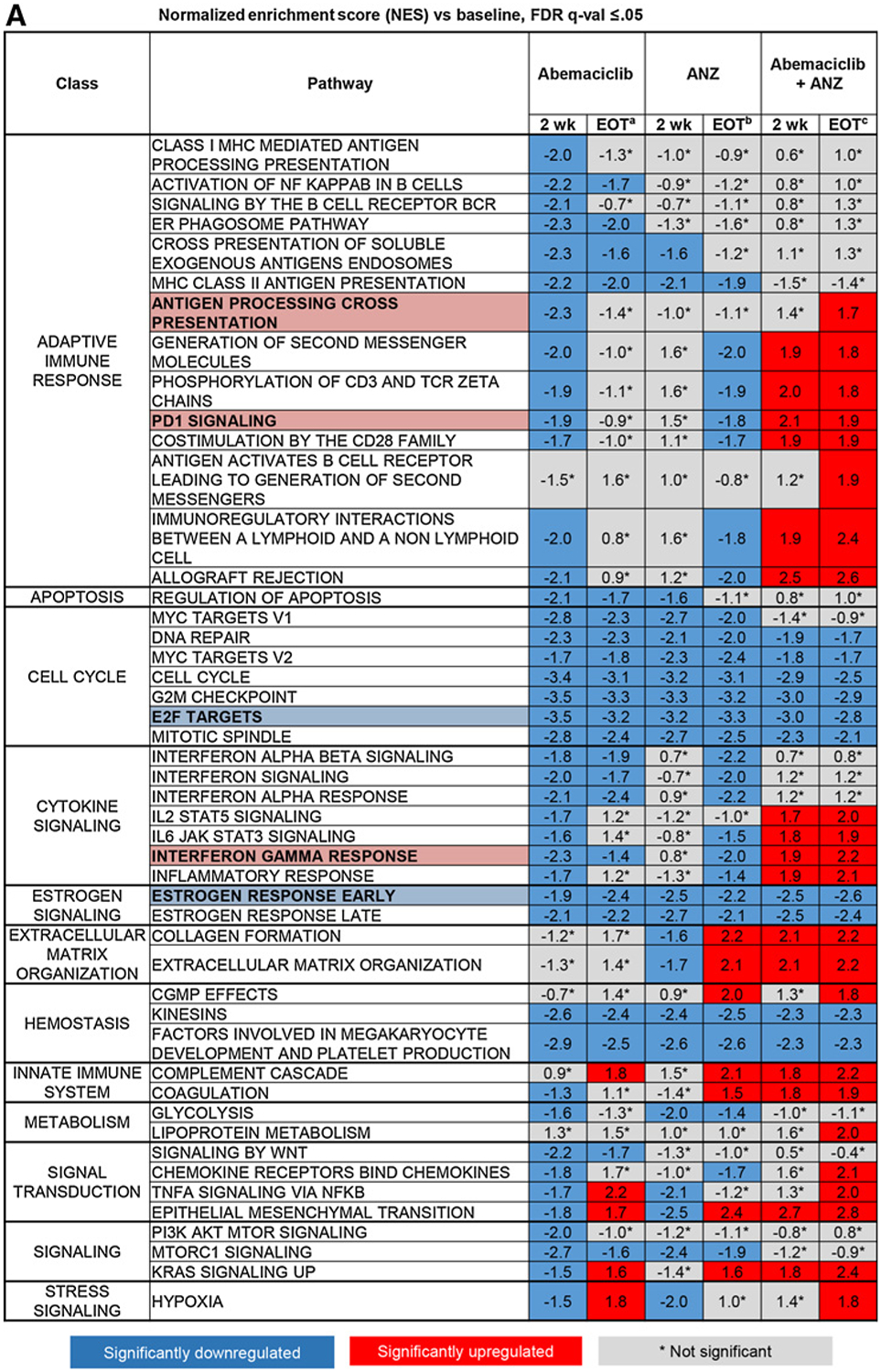
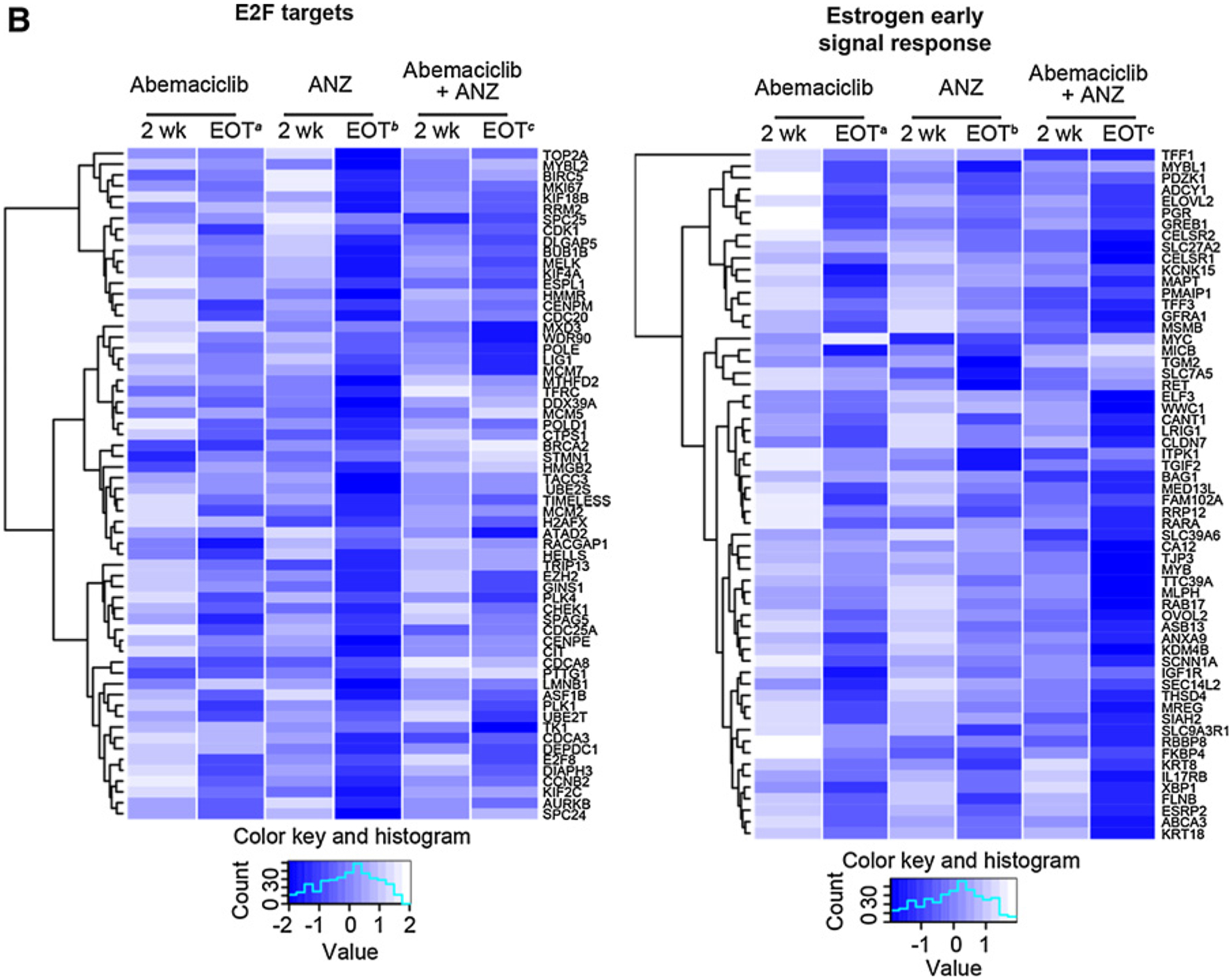
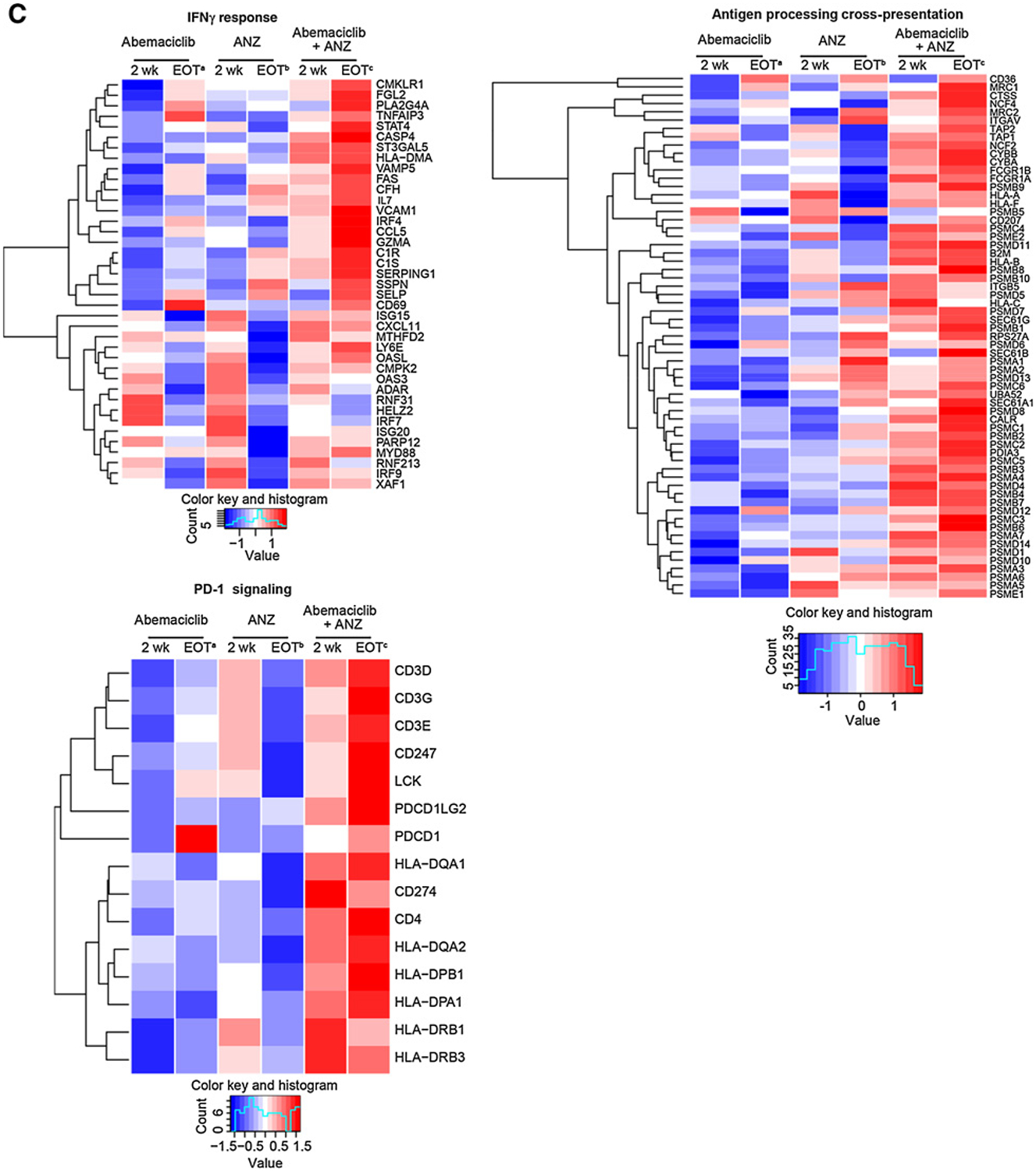
Results: Abemaciclib, alone or in combination with anastrozole, achieved a significant decrease in Ki67 expression and led to potent cell-cycle arrest after 2 weeks of treatment compared with anastrozole alone. More patients in the abemaciclib-containing arms versus anastrozole alone achieved complete cell-cycle arrest (58%/68% vs. 14%, P < 0.001). At the end of treatment, following 2 weeks lead-in and 14 weeks of combination therapy, 46% of intent-to-treat patients achieved a radiologic response, with pathologic complete response observed in 4%. The most common all-grade adverse events were diarrhea (62%), constipation (44%), and nausea (42%). Abemaciclib, anastrozole, and the combination inhibited cell-cycle processes and estrogen signaling; however, combination therapy resulted in increased cytokine signaling and adaptive immune response indicative of enhanced antigen presentation and activated T-cell phenotypes.
Conclusions: Abemaciclib plus anastrozole demonstrated biological and clinical activity with generally manageable toxicities in patients with HR+/HER2- early breast cancer. Abemaciclib led to potent cell-cycle arrest, and in combination with anastrozole, enhanced immune activation.
Trial registration: ClinicalTrials.gov NCT02441946.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
S.A. Hurvitz reports receiving commercial research grants from Ambrx, Amgen, Bayer, Boehringer-Ingelheim, Daiichi-Sankyo, Genentech/Roche, GlaxoSmithKline, Immunomedics, Lilly, Novartis, Pfizer, Macrogenics, OBI Pharma, Pieris, PUMA, Sanofi, Seattle Genetics, Medivation, and Merrimack, and is an advisory board member/unpaid consultant for GlaxoSmithKline, Novartis, AstraZeneca, Lilly, Amgen, and Daiichi Sankyo. M. Martin is a paid consultant for Roche, Novartis, PUMA, AstraZeneca, Amgen, Taiho Oncology, Pharmamar, Eli Lilly, and Daiichi Sankyo, and reports receiving commercial research grants from Roche, Novartis, and PUMA. M.F. Press is a paid consultant for Biocartis, Puma Biotechnology, Cepheid, Karyopharm Therapeutics, Science Branding Communications, Novartis, and Zymeworks, Inc., and reports receiving commercial research grants from Cepheid, Eli Lilly, F. Hoffmann-La Roche AG, and Novartis, and other remuneration from Amgen, Inc. M. Fernandez-Abad is an advisory board member/unpaid consultant for Eli Lilly. E. Petru is an advisory board member/unpaid consultant for Abemaciclib. V. Guarneri reports receiving speakers bureau honoraria from and is an advisory board member/unpaid consultant for Eli Lilly. C. Huang reports receiving commercial research grants from Eli Lilly; other commercial research support from Roche, Novartis, MSD, EirGenix, OBI Pharma, Daiichi Sankyo, AstraZeneca, and Pfizer; and speakers bureau honoraria from Amgen, Pfizer, Roche, and Novartis, and is an advisory board member/unpaid consultant for Eli Lilly, Pfizer, Roche, and Amgen. S. Barriga, P.J. Ebert, A. Aggarwal, and V.M. Jansen are employees/paid consultants for and hold ownership interest (including patents) in Eli Lilly. S.R. Wijayawardana, A. Hossain, and J. Liu are employees/paid consultants for Eli Lilly. D.J. Slamon is a paid consultant for Eli Lilly, Novartis, and Pfizer; reports receiving commercial research grants from Novartis; and holds ownership interest (including patents) in Pfizer, Amgen, Seattle Genetics, and BioMarin. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Howell A, Cuzick J, Baum M, Buzdar A, Dowsett M, Forbes JF, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet 2005;365:60–2. - PubMed
-
- Finn RS, Crown JP, Lang I, Boer K, Bondarenko IM, Kulyk SO, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncolo 2015;16:25–35. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
