

Genome-wide CRISPR/Cas9 library screening identified PHGDH as a critical driver for Sorafenib resistance in HCC
- PMID: 31615983
- PMCID: PMC6794322
- DOI: 10.1038/s41467-019-12606-7
Genome-wide CRISPR/Cas9 library screening identified PHGDH as a critical driver for Sorafenib resistance in HCC
Abstract
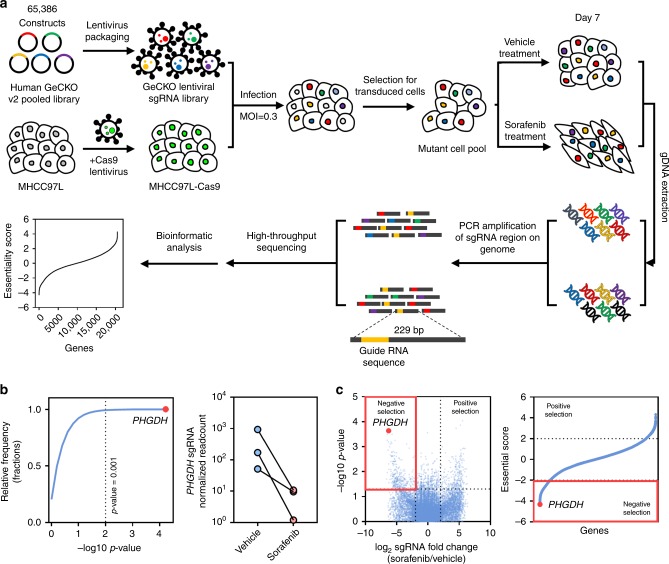
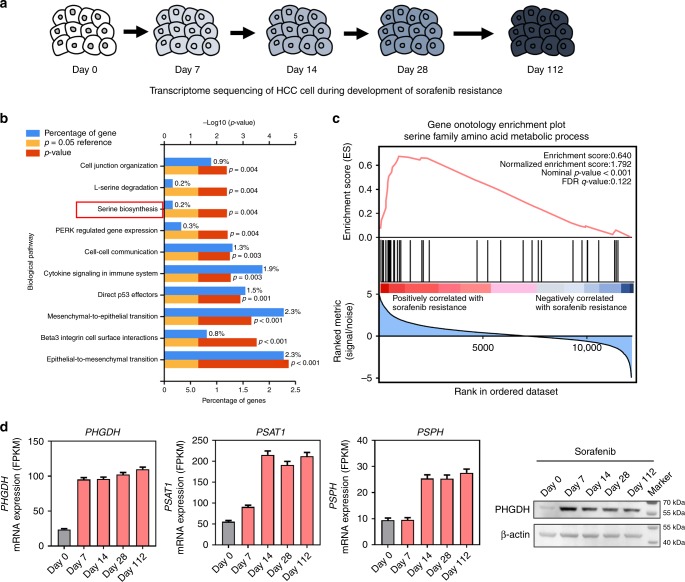
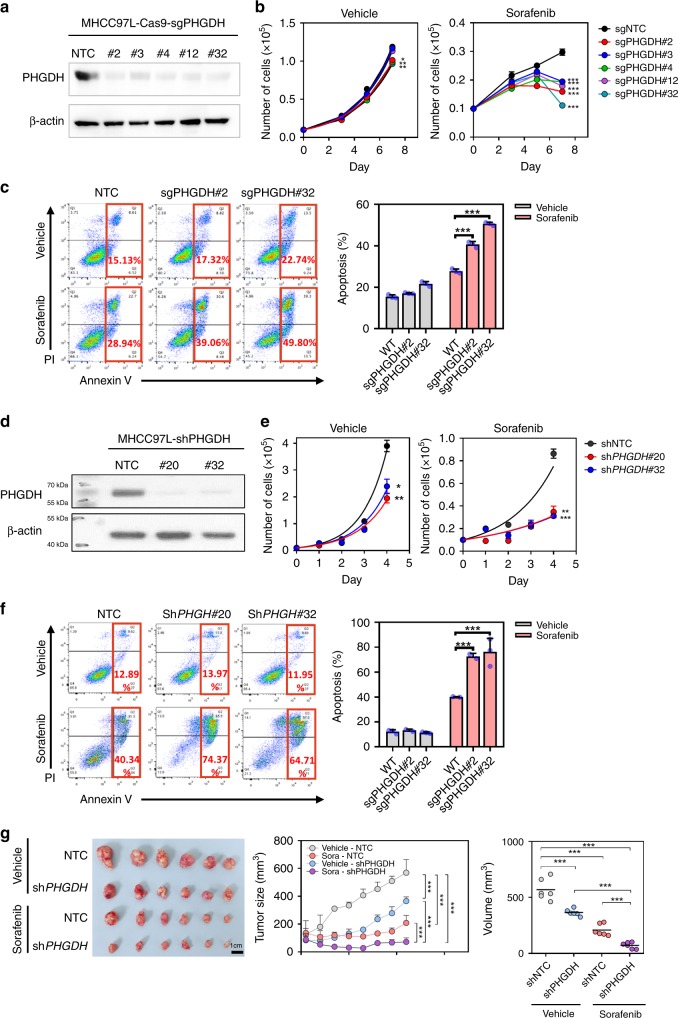
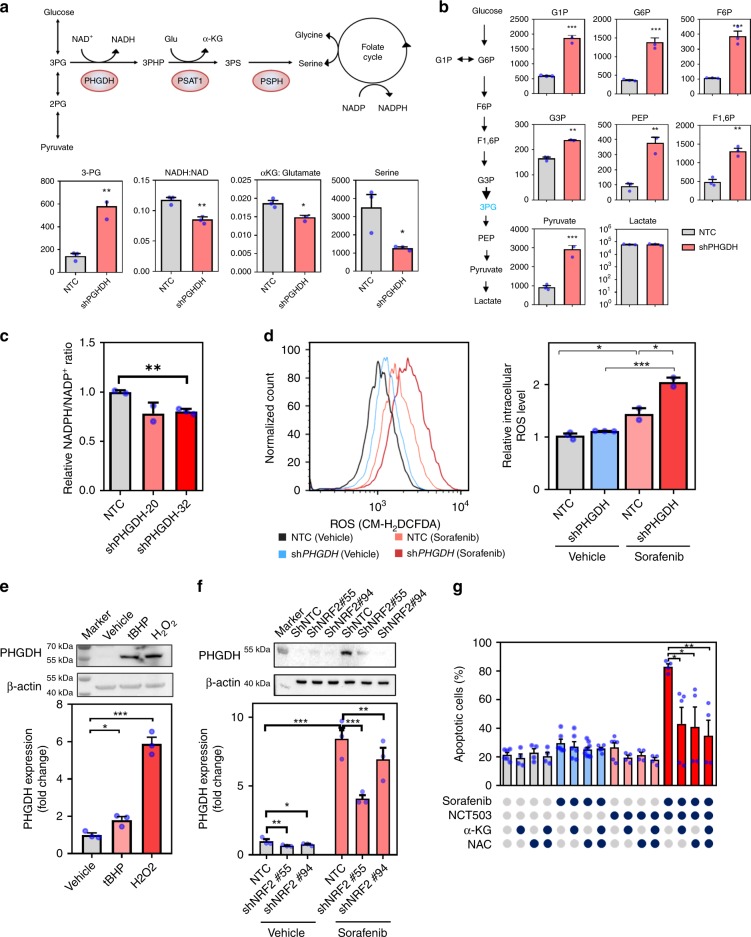
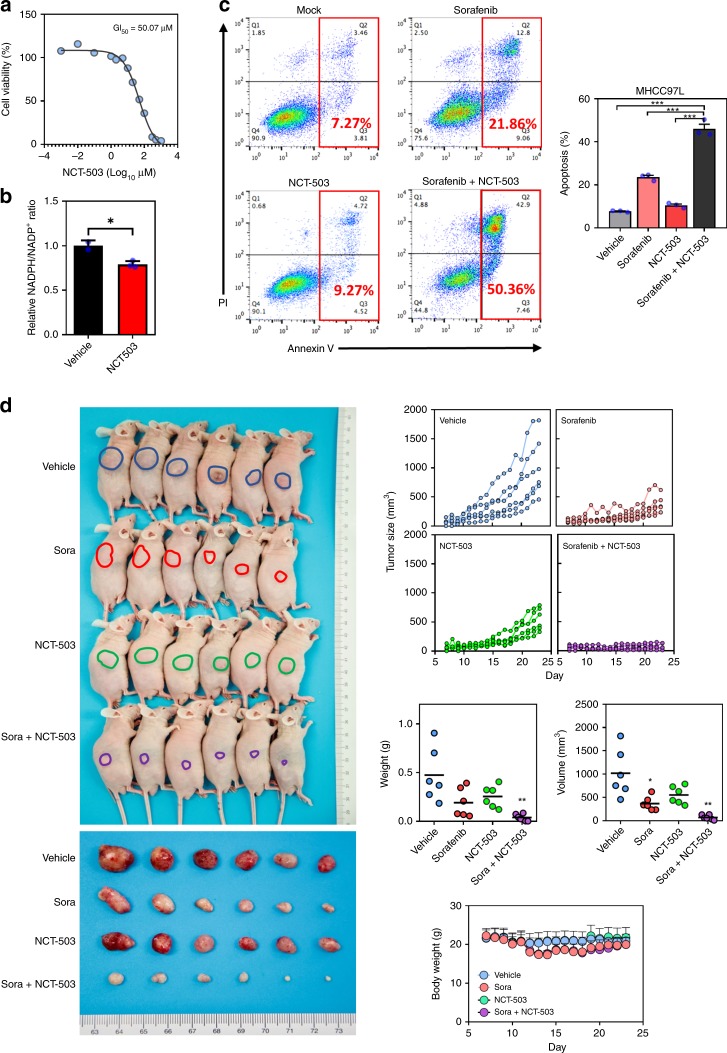
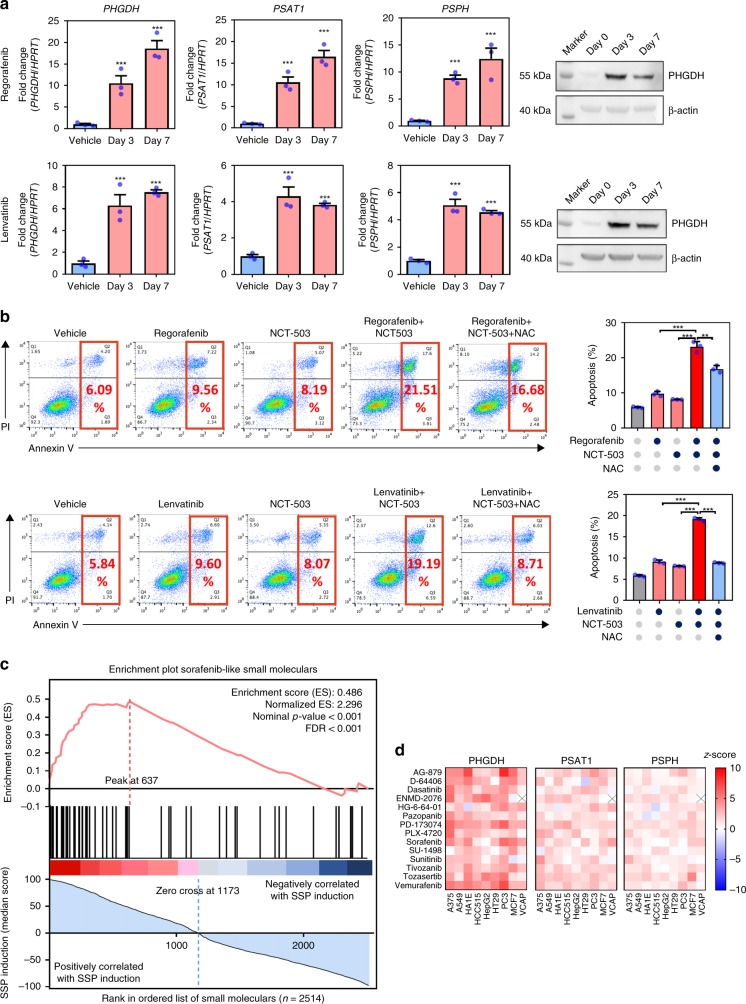
Sorafenib is the standard treatment for advanced hepatocellular carcinoma (HCC). However, the development of drug resistance is common. By using genome-wide CRISPR/Cas9 library screening, we identify phosphoglycerate dehydrogenase (PHGDH), the first committed enzyme in the serine synthesis pathway (SSP), as a critical driver for Sorafenib resistance. Sorafenib treatment activates SSP by inducing PHGDH expression. With RNAi knockdown and CRISPR/Cas9 knockout models, we show that inactivation of PHGDH paralyzes the SSP and reduce the production of αKG, serine, and NADPH. Concomitantly, inactivation of PHGDH elevates ROS level and induces HCC apoptosis upon Sorafenib treatment. More strikingly, treatment of PHGDH inhibitor NCT-503 works synergistically with Sorafenib to abolish HCC growth in vivo. Similar findings are also obtained in other FDA-approved tyrosine kinase inhibitors (TKIs), including Regorafenib or Lenvatinib. In summary, our results demonstrate that targeting PHGDH is an effective approach to overcome TKI drug resistance in HCC.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
