

Cardiovascular Risk in Fatty Liver Disease: The Liver-Heart Axis-Literature Review
- PMID: 31616668
- PMCID: PMC6763690
- DOI: 10.3389/fmed.2019.00202
Cardiovascular Risk in Fatty Liver Disease: The Liver-Heart Axis-Literature Review
Abstract
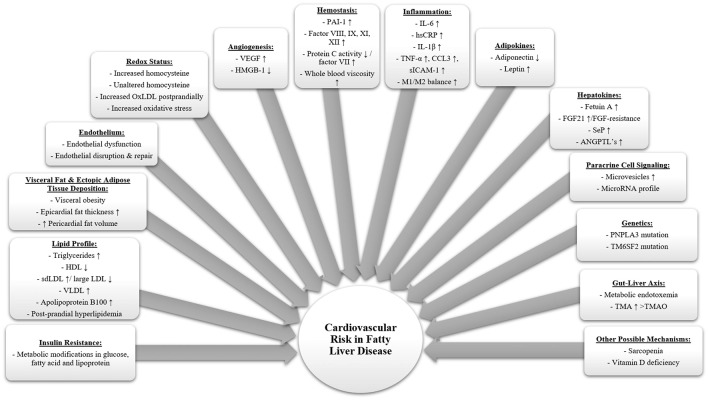
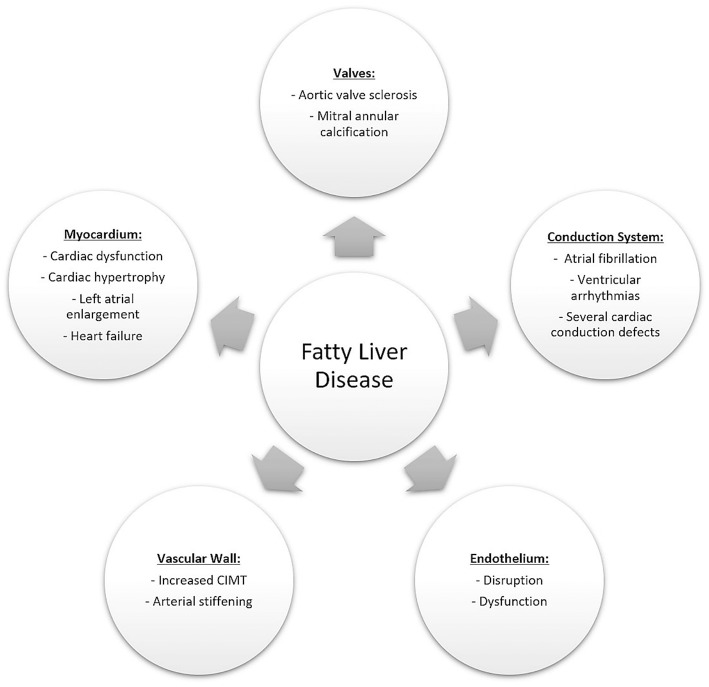
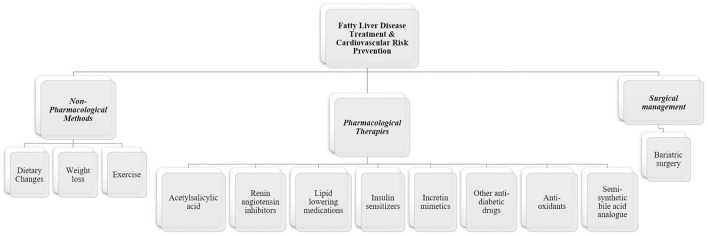
According to the World Health Organization, cardiovascular disease (CVD) remains the leading cause of death worldwide, accounting for approximately 18 million deaths per year. Nevertheless, the worldwide prevalence of metabolic diseases, such as type 2 diabetes mellitus, obesity, and non-alcoholic fatty liver disease (NAFLD), also known to be common risk factors for CVD, have dramatically increased over the last decades. Chronic alcohol consumption is a major cause of chronic liver diseases (CLD) as well as being a major health care cost expenditure accounting for the spending of tremendous amounts of money annually. NAFLD has become one of the major diseases plaguing the world while standing as the most common cause of liver disease in the Western countries by representing about 75% of all CLD. Currently, the most common cause of death in NAFLD remains to be CVD. Several mechanisms have been suggested to be responsible for associating FLD with CVD through several mechanisms including low-grade systemic inflammation, oxidative stress, adipokines, endoplasmic reticulum stress, lipotoxicity and microbiota dysbiosis which may also be influenced by other factors such as genetic and epigenetic variations. Despite of all this evidence, the exact mechanisms of how FLD can causally contribute to CVD are not fully elucidated and much remains unknown. Moreover, the current literature supports the increasing evidence associating FLD with several cardiovascular (CV) adverse events including coronary artery disease, increased subclinical atherosclerosis risk, structural alterations mainly left ventricular hypertrophy, increased epicardial fat thickness, valvular calcifications including aortic valve sclerosis and mitral annular calcification and functional cardiac modifications mainly diastolic dysfunction in addition to cardiac arrhythmias such as atrial fibrillation and ventricular arrythmias and conduction defects including atrioventricular blocks and bundle branch blocks. Patients with FLD should be evaluated and managed accordingly in order to prevent further complications. Possible management methods include non-pharmacological strategies including life style modifications, pharmacological therapies as well as surgical management. This review aims to summarize the current state of knowledge regarding the pathophysiological mechanisms linking FLD with an increased CV risk, in addition to associated CV adverse events and current management modalities.
Keywords: alcoholic liver disease (ALD); cardiac arrhythmias; cardiovascular disease (CV disease); metabolic syndrome (MetS); non-alcoholic fatty liver disease (NAFLD).
Copyright © 2019 Ismaiel and Dumitraşcu.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical