

Evolution of Spinal Endoscopic Surgery
- PMID: 31618807
- PMCID: PMC6449828
- DOI: 10.14245/ns.1836322.161
Evolution of Spinal Endoscopic Surgery
Abstract
Innovations in the development of endoscopic spinal surgery were classified into different generations and reviewed. Future developments and directions for endoscopic spinal surgery were discussed. Surgical therapy for spinal disease has been gradually changing from traditional open surgery to minimally invasive spinal surgery. Recently, endoscopic spinal surgery, which initially was limited to the treatment of soft tissue lesions, has expanded to include other aspects of spinal disease and good clinical results have been reported. As the paradigm of spinal surgery shifts from open surgery to endoscopic surgery, we discussed the evolution of endoscopic spine surgery in our literature review. Through this description, we presented possibilities of future developments and directions in endoscopic spine surgery.
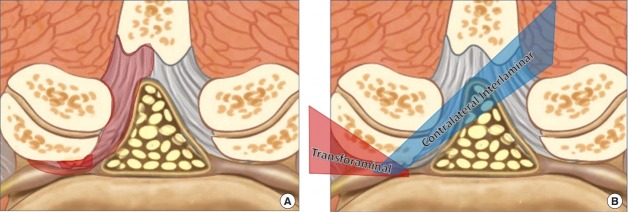
Keywords: Endoscopic spinal surgery; Interlaminar approach; Percutaneous spinal surgery; Transforaminal approach.
Conflict of interest statement
The authors have nothing to disclose.
Figures

References
-
- Ishimoto Y, Yoshimura N, Muraki S, et al. Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population-based cohort in Japan: the Wakayama Spine Study. Osteoarthritis Cartilage. 2012;20:1103–8. - PubMed
-
- Ahn Y. Percutaneous endoscopic decompression for lumbar spinal stenosis. Expert Rev Med Devices. 2014;11:605–16. - PubMed
-
- Gibson JN, Cowie JG, Iprenburg M. Transforaminal endoscopic spinal surgery: the future 'gold standard' for discectomy? - A review. Surgeon. 2012;10:290–6. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
