

Customized versus population birth weight charts for identification of newborns at risk of long-term adverse cardio-metabolic and respiratory outcomes: a population-based prospective cohort study
- PMID: 31619225
- PMCID: PMC6796410
- DOI: 10.1186/s12916-019-1424-4
Customized versus population birth weight charts for identification of newborns at risk of long-term adverse cardio-metabolic and respiratory outcomes: a population-based prospective cohort study
Abstract
Background: Customized birth weight charts take into account physiological maternal characteristics that are known to influence fetal growth to differentiate between physiological and pathological abnormal size at birth. It is unknown whether customized birth weight charts better identify newborns at risk of long-term adverse outcomes than population birth weight charts. We aimed to examine whether birth weight classification according to customized charts is superior to population charts at identification of newborns at risk of adverse cardio-metabolic and respiratory health outcomes.
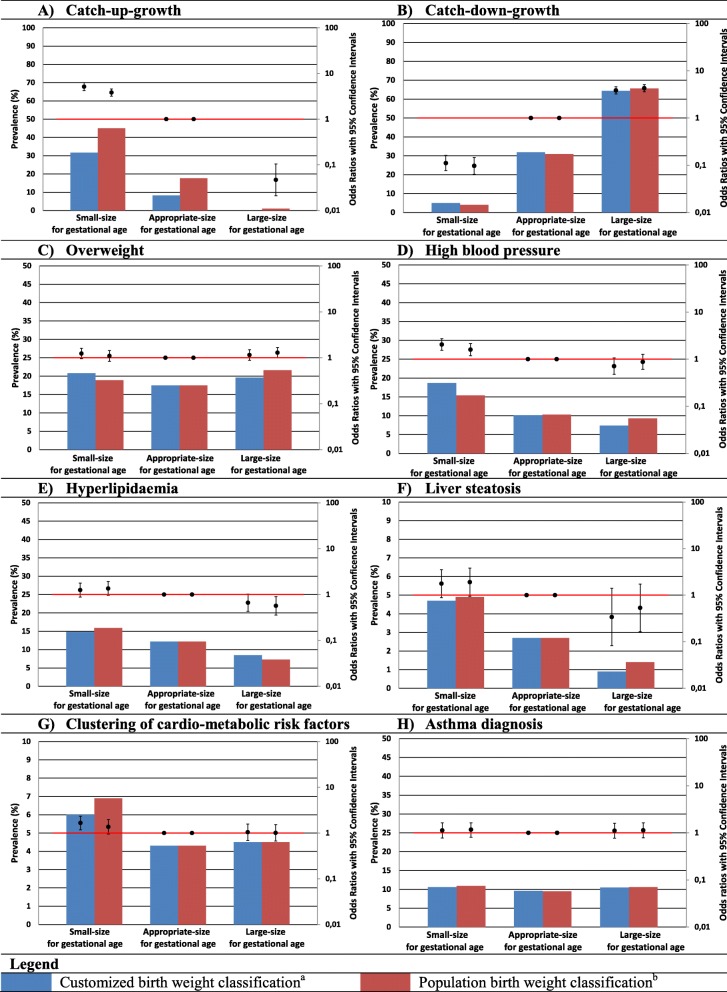
Methods: In a population-based prospective cohort study among 6052 pregnant women and their children, we measured infant catch-up growth, overweight, high blood pressure, hyperlipidemia, liver steatosis, clustering of cardio-metabolic risk factors, and asthma at age 10. Small size and large size for gestational age at birth was defined as birth weight in the lowest or highest decile, respectively, of population or customized charts. Association with birth weight classification was assessed using logistic regression models.
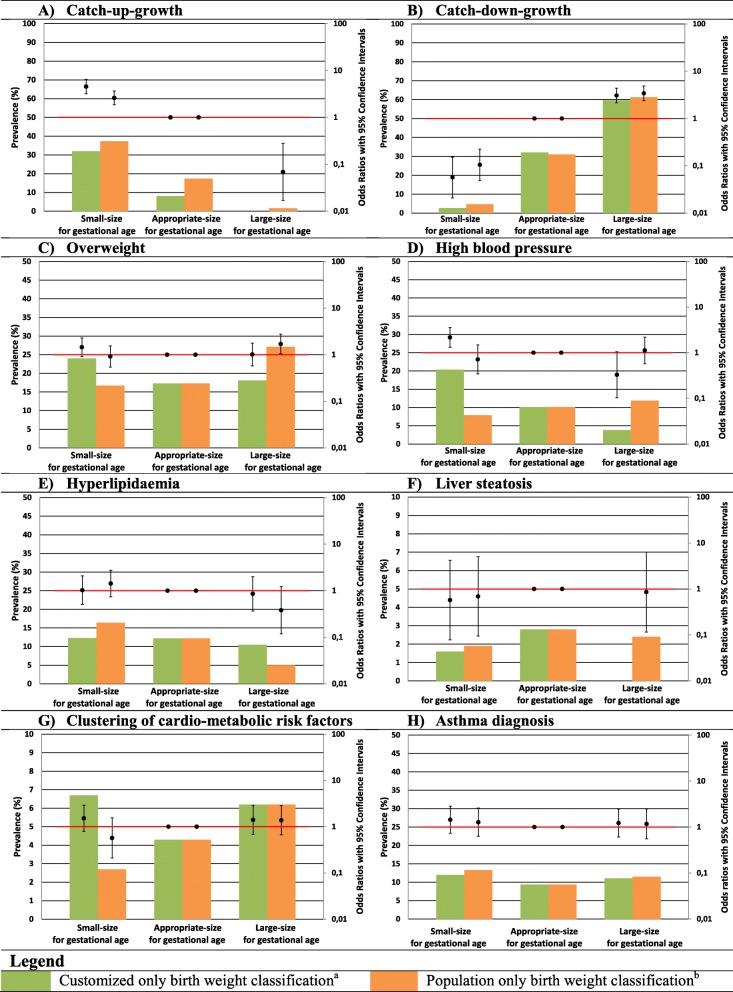
Results: Of the total of 605 newborns classified as small size for gestational age by population charts, 150 (24.8%) were reclassified as appropriate size for gestational age by customized charts, whereas of the total of 605 newborns classified as large size for gestational age by population charts, 129 (21.3%) cases were reclassified as appropriate size for gestational age by customized charts. Compared to newborns born appropriate size for gestational age, newborns born small size for gestational age according to customized charts had increased risks of infant catch-up growth (odds ratio (OR) 5.15 (95% confidence interval (CI) 4.22 to 6.29)), high blood pressure (OR 2.05 (95% CI 1.55 to 2.72)), and clustering of cardio-metabolic risk factors at 10 years (OR 1.66 (95% CI 1.18 to 2.34)). No associations were observed for overweight, hyperlipidemia, liver steatosis, or asthma. Newborns born large-size for gestational age according to customized charts had higher risk of catch-down-growth only (OR 3.84 (95% CI 3.22 to 4.59)). The direction and strength of the observed associations were largely similar when we used classification according to population charts.
Conclusions: Small-size-for-gestational-age newborns seem to be at risk of long-term adverse cardio-metabolic health outcomes, irrespective of the use of customized or population birth weight charts.
Keywords: Birth weight; Cardiovascular health; Charts; Child; Customization; Outcomes; Respiratory health.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Press R. RCOG Press at the Royal College of Obsstetricians and Gynaecologists. 2008. Antenatal care: Routine care for the healthy pregnant woman. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
