Comprehensive understanding of vascular anatomy for endovascular treatment of intractable oronasal bleeding
- PMID: 31620565
- PMCID: PMC6784680
- DOI: 10.12701/yujm.2018.35.1.7
Comprehensive understanding of vascular anatomy for endovascular treatment of intractable oronasal bleeding
Abstract
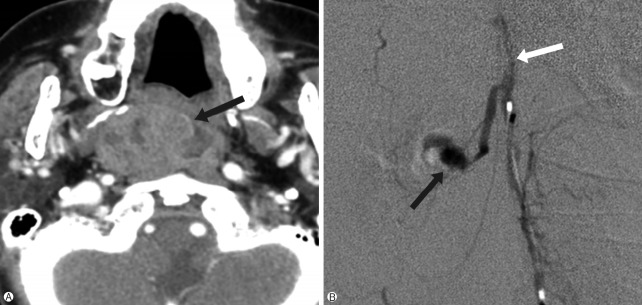
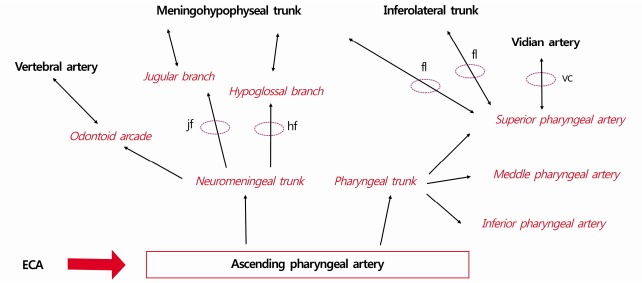
Oronasal bleeding that continues despite oronasal packs or recurs after removal of the oronasal packs is referred to as intractable oronasal bleeding, which is refractory to conventional treatments. Severe craniofacial injury or tumor in the nasal or paranasal cavity may cause intractable oronasal bleeding. These intractable cases are subsequently treated with surgical ligation or endovascular embolization of the bleeding arteries. While endovascular embolization has several merits compared to surgical ligation, the procedure needs attention because severe complications such as visual disturbance or cerebral infarction can occur. Therefore, comprehensive understanding of the head and neck vascular anatomy is essential for a more effective and safer endovascular treatment of intractable oronasal bleeding.
Keywords: Bleeding; Embolization; Epistaxis; External carotid artery; Intractable.
Copyright © 2018 Yeungnam University College of Medicine.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures









Similar articles
-
Endovascular treatment of intractable oronasal bleeding associated with severe craniofacial injury.J Trauma. 1998 Feb;44(2):330-4. doi: 10.1097/00005373-199802000-00017. J Trauma. 1998. PMID: 9498506
-
Transarterial embolization for traumatic intractable oronasal hemorrhage.J Emerg Med. 2013 Jun;44(6):1088-91. doi: 10.1016/j.jemermed.2012.06.029. Epub 2013 Jan 16. J Emerg Med. 2013. PMID: 23332804
-
[Management of intractable epistaxis and bleeding points localization of post-therapy nasopharyngeal carcinoma].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2012 Mar;47(3):191-5. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2012. PMID: 22805018 Chinese.
-
Clinical Practice Guideline: Nosebleed (Epistaxis) Executive Summary.Otolaryngol Head Neck Surg. 2020 Jan;162(1):8-25. doi: 10.1177/0194599819889955. Otolaryngol Head Neck Surg. 2020. PMID: 31910122 Review.
-
Endovascular management of internal carotid artery injuries secondary to endonasal surgery: case series and review of the literature.J Neurosurg. 2016 Nov;125(5):1256-1276. doi: 10.3171/2015.6.JNS142483. Epub 2016 Jan 15. J Neurosurg. 2016. PMID: 26771847 Review.
Cited by
-
The Nasopharyngo-Septal Butterfly Flap: A Novel Adjunct for Reconstructing Large Skull Base Defects.OTO Open. 2024 Oct 30;8(4):e70016. doi: 10.1002/oto2.70016. eCollection 2024 Oct-Dec. OTO Open. 2024. PMID: 39478729 Free PMC article.
-
Woodruff's plexus-arterial or venous?Surg Radiol Anat. 2022 Jan;44(1):169-181. doi: 10.1007/s00276-021-02852-0. Epub 2021 Oct 29. Surg Radiol Anat. 2022. PMID: 34714375
References
-
- Small M, Murray JA, Maran AG. A study of patients with epistaxis requiring admission to hospital. Health Bull (Edinb) 1982;40:20–9. - PubMed
-
- Pallin DJ, Chng YM, McKay MP, Emond JA, Pelletier AJ, Camargo CA., Jr Epidemiology of epistaxis in US emergency departments, 1992 to 2001. Ann Emerg Med. 2005;46:77–81. - PubMed
-
- Walker TW, Macfarlane TV, McGarry GW. The epidemiology and chronobiology of epistaxis: an investigation of Scottish hospital admissions 1995-2004. Clin Otolaryngol. 2007;32:361–5. - PubMed
-
- Tan LK, Calhoun KH. Epistaxis. Med Clin North Am. 1999;83:43–56. - PubMed
-
- Viducich RA, Blanda MP, Gerson LW. Posterior epistaxis: clinical features and acute complications. Ann Emerg Med. 1995;25:592–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources