

Use of MIRUS™ for MAC-driven application of isoflurane, sevoflurane, and desflurane in postoperative ICU patients: a randomized controlled trial
- PMID: 31620921
- PMCID: PMC6795651
- DOI: 10.1186/s13613-019-0594-8
Use of MIRUS™ for MAC-driven application of isoflurane, sevoflurane, and desflurane in postoperative ICU patients: a randomized controlled trial
Abstract
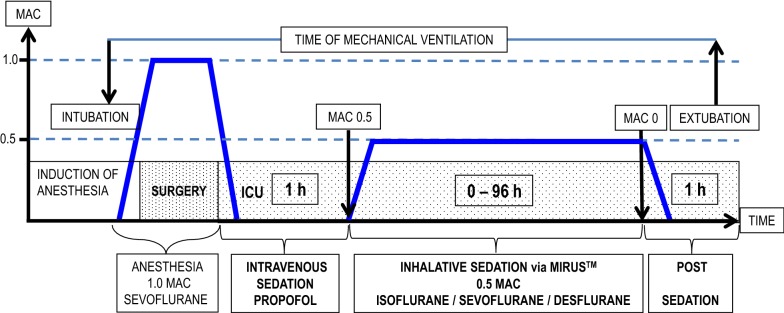
Background: The MIRUS™ (TIM, Koblenz, Germany) is an electronical gas delivery system, which offers an automated MAC (minimal alveolar concentration)-driven application of isoflurane, sevoflurane, or desflurane, and can be used for sedation in the intensive care unit. We investigated its consumption of volatile anesthetics at 0.5 MAC (primary endpoint) and the corresponding costs. Secondary endpoints were the technical feasibility to reach and control the MAC automatically, the depth of sedation at 0.5 MAC, and awakening times. Mechanically ventilated and sedated patients after major surgery were enrolled. Upon arrival in the intensive care unit, patients obtained intravenous propofol sedation for at least 1 h to collect ventilation and blood gas parameters, before they were switched to inhalational sedation using MIRUS™ with isoflurane, sevoflurane, or desflurane. After a minimum of 2 h, inhalational sedation was stopped, and awakening times were recorded. A multivariate electroencephalogram and the Richmond Agitation Sedation Scale (RASS) were used to assess the depth of sedation. Vital signs, ventilation parameters, gas consumption, MAC, and expiratory gas concentrations were continuously recorded.
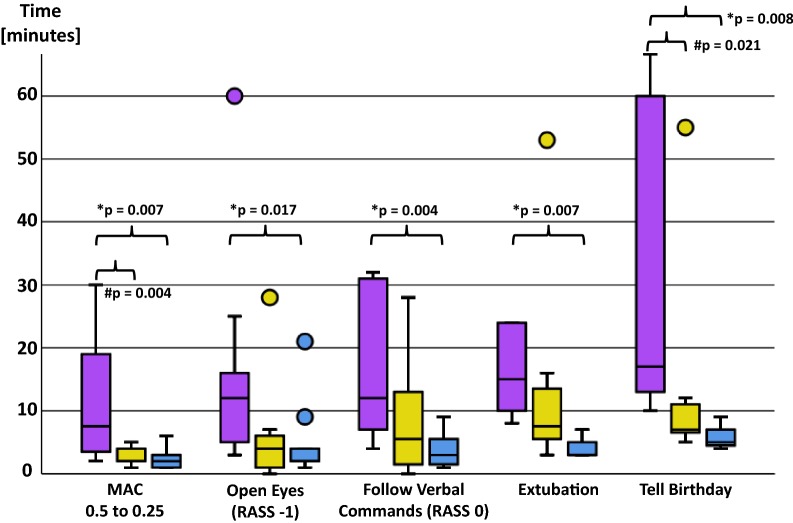
Results: Thirty patients obtained inhalational sedation for 18:08 [14:46-21:34] [median 1st-3rd quartiles] hours. The MAC was 0.58 [0.50-0.64], resulting in a Narcotrend Index of 37.1 [30.9-42.4] and a RASS of - 3.0 [- 4.0 to (- 3.0)]. The median gas consumption was significantly lowest for isoflurane ([ml h-1]: isoflurane: 3.97 [3.61-5.70]; sevoflurane: 8.91 [6.32-13.76]; and desflurane: 25.88 [20.38-30.82]; p < 0.001). This corresponds to average costs of 0.39 € h-1 for isoflurane, 2.14 € h-1 for sevoflurane, and 7.54 € h-1 for desflurane. Awakening times (eye opening [min]: isoflurane: 9:48 [4:15-20:18]; sevoflurane: 3:45 [0:30-6:30]; desflurane: 2:00 [1:00-6:30]; p = 0.043) and time to extubation ([min]: isoflurane: 10:10 [8:00-20:30]; sevoflurane: 7:30 [4:37-14:22]; desflurane: 3:00 [3:00-6:00]; p = 0.007) were significantly shortest for desflurane.
Conclusions: A target-controlled, MAC-driven automated application of volatile anesthetics is technically feasible and enables an adequate depth of sedation. Gas consumption was highest for desflurane, which is also the most expensive volatile anesthetic. Although awakening times were shortest, the actual time saving of a few minutes might be negligible for most patients in the intensive care unit. Thus, using desflurane seems not rational from an economic perspective. Trial registration Clinical Trials Registry (ref.: NCT03860129). Registered 24 September 2018-Retrospectively registered.
Keywords: Desflurane; Inhalational sedation; Isoflurane; MAC-driven sedation; Sevoflurane.
Conflict of interest statement
MB, AM, and JH-N received speakers’ honoraria from Pall Medical, Dreieich, Germany, the former owner of the MIRUS System in 2017 (1200 € each). The other authors declare that they have no competing interests.
Figures
References
-
- Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825–e873. doi: 10.1097/CCM.0000000000003299. - DOI - PubMed
-
- Jerath A, Panckhurst J, Parotto M, Lightfoot N, Wasowicz M, Ferguson ND, et al. Safety and efficacy of volatile anesthetic agents compared with standard intravenous midazolam/propofol sedation in ventilated critical care patients: a meta-analysis and systematic review of prospective trials. Anesth Analg. 2017;124:1190–1199. doi: 10.1213/ANE.0000000000001634. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
