

Prospective evaluation of oral premalignant lesions using a multimodal imaging system: a pilot study
- PMID: 31621979
- PMCID: PMC7003735
- DOI: 10.1002/hed.25978
Prospective evaluation of oral premalignant lesions using a multimodal imaging system: a pilot study
Abstract
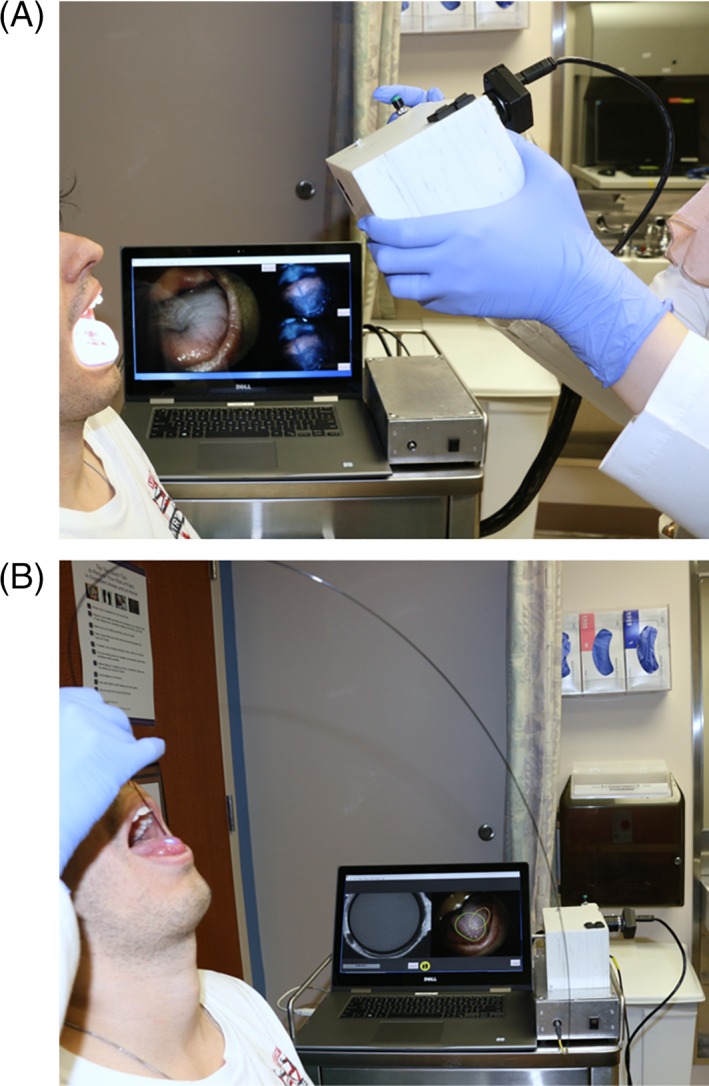
Background: Multimodal optical imaging, incorporating reflectance and fluorescence modalities, is a promising tool to detect oral premalignant lesions in real-time.
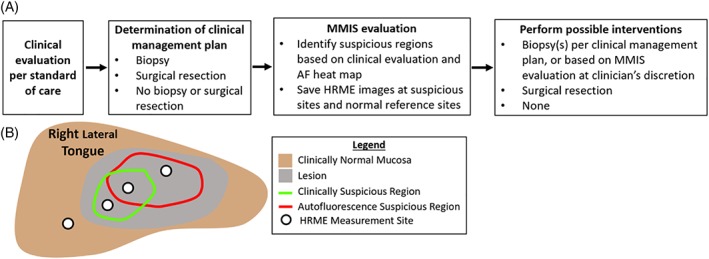
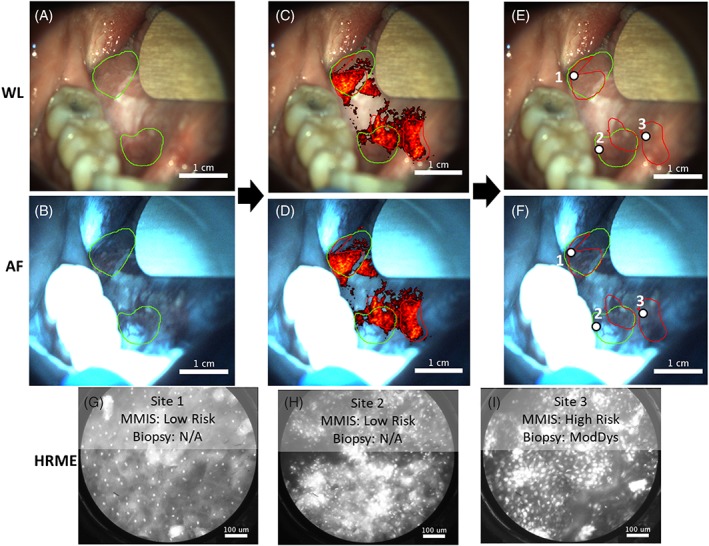
Methods: Images were acquired from 171 sites in 66 patient visits for clinical evaluation of oral lesions. An automated algorithm was used to classify lesions as high- or low-risk for neoplasia. Biopsies were acquired at clinically indicated sites and those classified as high-risk by imaging, at the surgeon's discretion.
Results: Twenty sites were biopsied based on clinical examination or imaging. Of these, 12 were indicated clinically and by imaging; 58% were moderate dysplasia or worse. Four biopsies were indicated by imaging evaluation only; 75% were moderate dysplasia or worse. Finally, four biopsies were indicated by clinical evaluation only; 75% were moderate dysplasia or worse.
Conclusion: Multimodal imaging identified more cases of high-grade dysplasia than clinical evaluation, and can improve detection of high grade precancer in patients with oral lesions.
Keywords: cancer; image analysis; optical imaging; oral lesion; prevention.
© 2019 The Authors. Head & Neck published by Wiley Periodicals, Inc.
Figures
Similar articles
-
Prospective Evaluation of Multimodal Optical Imaging with Automated Image Analysis to Detect Oral Neoplasia In Vivo.Cancer Prev Res (Phila). 2017 Oct;10(10):563-570. doi: 10.1158/1940-6207.CAPR-17-0054. Epub 2017 Aug 1. Cancer Prev Res (Phila). 2017. PMID: 28765195 Free PMC article.
-
Development of an integrated multimodal optical imaging system with real-time image analysis for the evaluation of oral premalignant lesions.J Biomed Opt. 2019 Feb;24(2):1-10. doi: 10.1117/1.JBO.24.2.025003. J Biomed Opt. 2019. PMID: 30793567 Free PMC article.
-
In Vivo Multimodal Optical Imaging: Improved Detection of Oral Dysplasia in Low-Risk Oral Mucosal Lesions.Cancer Prev Res (Phila). 2018 Aug;11(8):465-476. doi: 10.1158/1940-6207.CAPR-18-0032. Epub 2018 Jun 14. Cancer Prev Res (Phila). 2018. PMID: 29903741 Free PMC article. Clinical Trial.
-
Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: current limitations and future directions.Oral Surg Oral Med Oral Pathol Oral Radiol. 2018 Jun;125(6):670-681. doi: 10.1016/j.oooo.2018.02.020. Epub 2018 Mar 9. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018. PMID: 29631985 Free PMC article. Review.
-
Flow cytometer analysis of oral premalignant lesions: a pilot study and review.J Oral Pathol Med. 1992 Jan;21(1):1-6. doi: 10.1111/j.1600-0714.1992.tb00959.x. J Oral Pathol Med. 1992. PMID: 1375642 Review.
Cited by
-
Optical imaging technologies for in vivo cancer detection in low-resource settings.Curr Opin Biomed Eng. 2023 Dec;28:100495. doi: 10.1016/j.cobme.2023.100495. Epub 2023 Aug 23. Curr Opin Biomed Eng. 2023. PMID: 38406798 Free PMC article.
-
Algorithm to quantify nuclear features and confidence intervals for classification of oral neoplasia from high-resolution optical images.J Med Imaging (Bellingham). 2020 Sep;7(5):054502. doi: 10.1117/1.JMI.7.5.054502. Epub 2020 Sep 21. J Med Imaging (Bellingham). 2020. PMID: 32999894 Free PMC article.
-
Mildly dysplastic oral lesions with optically-detectable abnormalities share genetic similarities with severely dysplastic lesions.Oral Oncol. 2022 Dec;135:106232. doi: 10.1016/j.oraloncology.2022.106232. Epub 2022 Nov 3. Oral Oncol. 2022. PMID: 36335817 Free PMC article.
-
Multimodal optical imaging with real-time projection of cancer risk and biopsy guidance maps for early oral cancer diagnosis and treatment.J Biomed Opt. 2023 Jan;28(1):016002. doi: 10.1117/1.JBO.28.1.016002. Epub 2023 Jan 13. J Biomed Opt. 2023. PMID: 36654656 Free PMC article.
-
Unmet Needs and Perspectives in Oral Cancer Prevention.Cancers (Basel). 2022 Apr 2;14(7):1815. doi: 10.3390/cancers14071815. Cancers (Basel). 2022. PMID: 35406587 Free PMC article. Review.
References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer (2013). Available at: http://globocan.iarc.fr/Default.aspx
-
- Cancer of the Oral Cavity and Pharynx ‐ SEER Stat Fact Sheets. Available at: http://seer.cancer.gov/statfacts/html/oralcav.html.
-
- Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018;125:612‐627. - PubMed
-
- Jeong WJ, Paik JH, Cho SW, Sung MW, Kim KH, Ahn SH. Excisional biopsy for management of lateral tongue leukoplakia. J Oral Pathol Med. 2012;41:384‐388. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
